Download
1 / 30
300 likes | 536 Views
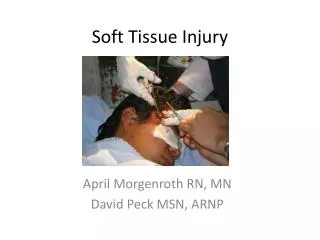
Venous vascular malformation type of soft tissue discovery at puberty. M . LAADHARI, A. AISSA, M. KHERIFECH, I. MEZHOUD, K. BEN HELAL*, M. ALLANI, R. ALOUINI Medical Imaging Ibn El Jazzar Hospital Kairouan * Department of Pediatrics Ibn El Jazzar Hospital Kairouan Tunisia

E N D
Venous vascular malformation type of soft tissue discovery at puberty M. LAADHARI, A. AISSA, M. KHERIFECH, I. MEZHOUD, K. BEN HELAL*, M. ALLANI, R. ALOUINI Medical Imaging Ibn El Jazzar Hospital Kairouan * Department of Pediatrics Ibn El Jazzar Hospital Kairouan Tunisia PAN ARAB 2012-PEDIATRICS : PD 9
Vascular malformations are a spectrum of unknown injury interesting mainly the pediatric population • Venous malformations are the most common vascular malformations • In case of complex or atypical clinical presentation, the doppler ultrasound and MRI are the two noninvasive imaging techniques which are essential : • To achieve the positive diagnosis towards differential diagnosis • To make an assessment of local and regional expansion referred to pre-therapeutic and prognostic and monitor spontaneous or on treatment of injuries INTRODUCTION
Illustrate a case of vascular malformation hemodynamically inactive venous type. • Demonstrate the role of different imaging means (standard X-ray, doppler ultrasound, cross-sectional imaging) in the diagnostic confirmation. OBJECTIVES
A 12-year-old patient without a historydisease, whichwaspresented to the ED with a painfulswelling of the forearm lasting for twodayswith a history of trauma twoweeksago. • Clinical examination: swelling of the medial surface soft, movable relative to the two planes, painful without cutaneous signs in regard. • An X-ray standard, a dopplerultrasound, a CT scan supplemented by an MRI were performed. OBSERVATION
OBSERVATION X-ray standard face of the forearm Soft tissue mass with round opacity tone calcium without adjacent bone changes.
OBSERVATION Doppler Ultra sound Multiple structures tubulated, tortuous hypoechoic, heterogeneous, infiltrating the subcutaneous fat, compressible with multiple hyperechoic spots followed by posterior acoustic shadowing (phlebolites). No flow at color Doppler and pulse.
OBSERVATION C T scann Lesion on the soft tissu, containing many heterogeneous hyperdensecalcifications of varying size, with enhancement after injection discreet locations.
OBSERVATION M R I(1,5T) Training oval in the subcutaneous and muscular tissue composed of contiguous structures serpiginousfranc hyperT2, isoT1 with intralesional structures in focal hypoT2 EG and T2 are compatible with phleboliths. Sequence -coronale -FSE T1- Sequence -coronale -STIR-
OBSERVATION M R I T1 T2 Sequence –axiale-FSE T1,FSET2 and T2* T2*
OBSERVATION M R I Axial-FSE T1 Fatsat after Gadolinium MIP Precoce and moderate enhancement, heterogeneous and "clumps" after injection. Coronal-FSE T1 Fatsat after Gadolinium
OBSERVATION M R I Coronal-FSE T1 Fatsat after Gadolinium
Prerequisite: know the classification of superficial vascular abnormalities. • Many sources of terminological confusion misdiagnosis and inappropriate treatment. DISCUSSION
DISCUSSION • VASCULAR TUMORS: abnormal endothelial cell proliferation • Vascular Malformations: embryological vessel abnormalities without abnormal cell proliferation Classification (1996) adopted by the International Society for the Study of Vascular Anomalies (ISSVA)
DISCUSSION Classification – Vascular tumor • Infantile hemangioma: the most common tumor in infants • Congenital hemangiomas (RICH and NICH), kaposiform hemangioendothelioma, tufted angioma • Exeptionnel: hemangiopericytoma, fibrosarcoma, rhabdomyosarcoma infant …
DISCUSSION Classification – Vascular malformations Classified according to hemodynamic data (classification more relevant) • Slow flow malformations (hemodynamically inactive): capillary,venous,lymphatic,combination of these malformations • Fast flow malformations (hemodynamically active): • Those with a blood component • Fistulaor arteriovenous malformation
DISCUSSION Vascular Malformation – General • Congenital lesions • Present at birth • Always sometimes late clinical manifestation (until adolescence) • Lack of spontaneous regression, persistence throughout life with growth proportional to that of the child • Possible phases of thrust if trauma, infection, hormonal changes (puberty, pregnancy)
DISCUSSION Vascular Malformation – General • Treatment usually necessary + + + • Treatment is conditioned by hemodynamic characteristics of the vascular malformations Importance of the distinction between congenital malformations and slow flow to fast flow
DISCUSSION A slow flux malformation of capillary type • Place of imaging very limited • Superficial anomaly hardly visible on imaging (sometimes skin thickening and subcutaneous) • Search for underlying vascular malformation or associated anomalies (vascular syndromes) + + +
DISCUSSION A slow flux malformation of Venous type • Most commonvascular malformation • Old"cavernoushemangioma" (confusingterminology) • Dysplasticveins: venousectasia or truevenouslakes (= cavitieswithvascularendotheliallining) • Oftenevidentatbirth • Oftenasymptomatic, sometimespainful if: • Thrust thrombosis secondary to intralesional or hormonal changes • Depth extension of the muscle • Joint damage Headquarters: head and neck region (40%), extremities (40%), trunk (20%)
DISCUSSION A slow flux malformation of Venous type Twocategories : Heredateryveinousmalformations Venous malformations common (our case) • The most common • Location : Cervicofacial+ + and members • Often later onset • Usual complications: thrombosis in situ always find a localized intravascular coagulation • Treatment only in cases of functional impairment or significant aesthetic
DISCUSSION A slow flux malformation of Venous type Members « Clinicalpresentation » • Possible with cutaneous, subcutaneous, muscle and joint • Pain due to thrombosis localized to gravity or nerve compression • In case of joint damage: recurrent effusions and hemorrhagic reaction with possible cartilage destruction (type hemophilic arthropathy)
DISCUSSION A slow flux malformation of Venous type « X-ray standard » • Mass of soft tissue • Non-specific but inconstant pathognomonic phleboliths (round opacities tone calcium) • Possible bone remodeling adjacent lesions extended
DISCUSSION A slow flux malformation of Venous type « Color and pulsed doppler ultrasound » Two types of venous malformations • Cavitary+++ • Gaps • Phlebolite • Slow venous flow monophasic • No flow (16%): thrombosis or technical limitations (very slow flow below the detection flux) => to Valsalvamaneuver • Component two-phase : flow capillary-associated (slow arterial flow) • Dysplasique • Multiple varicosedilatations • Multiple structures tubulées tortuous, anechoic, infiltrating the subcutaneous fat, muscle-tendon structures ... • Slow venousflow
DISCUSSION A slow flux malformation of Venous type « CT scann » • Little use • More sensitive than plain radiography for detecting phleboliths • Detection of any fatty component and detection of bone underlying
DISCUSSION A slow flux malformation of Venous type « IRM » PRECONISED PROTOCOLE • Importance of T2 FS or STIR sequences+ + + • SE T1 staging (anatomical balance), EG T2 (phleboliths, hemosiderin) • T1 FS gado (evaluation of perfusion) • 3D dynamic MR angiographywith injection • EG 3D T1 gadolinium bolus (2 ml / s) and subtraction • DynamicMRI: evaluation of time between the onset of arterialenhancement and earlyenhancement of the lesion : • Early if <or = 6 s: component malformation with arterial or capillary • Late if> 6 s : pure venous malformation
DISCUSSION A slow flux malformation of Venous type « IRM » HABITUEL ASPECTS • Serpiginousstructures, tubulatedor multilocular masses in connectionwithvenouslakesseparated by septa • Isosignal or hypo-signal on T1, frankhyper-signal on T2. • More heterogeneous signal on T1 if bleedingor thrombosis. • Hypo-signal areas on T2 (phleboliths, thrombi, septa). • Hypointense on all sequences (phleboliths). • EG asignalon T2 (slow flow). • Progressive enhancement"patchy" or "clumps" of circulatingareas.
DISCUSSION A slow flux malformation of Venous type « Per-cutanousphlebography » • Not useful for diagnosis • Stage 1 of treatment by sclerotherapy (in puncture of the malformation with needle 20-22 G) • Optimal evaluation of the anatomy of the MV and its venous drainage
The superficial vascular abnormalities are a diagnostic and therapeutic challenge that must be based on a multidisciplinary approach. • Their diagnosis is based primarily on clinical examination. • Vascular malformations are usually present at birth and do not regress spontaneously. CONCLUSION
Venous malformations are the most common vascular malformations and arteriovenous malformations are vascular malformations, the most dangerous, with unpredictable and difficult to treat. • It is important to distinguish between slow flow vascular malformations (capillary, venous, lymphatic) and vascular malformations fast flow (arteriovenous) that fall under different therapeutic management Interest of 3D MR angiography with dynamic gadolinium-enhanced and high temporal resolution (5 s). CONCLUSION