Download
1 / 15
160 likes | 369 Views
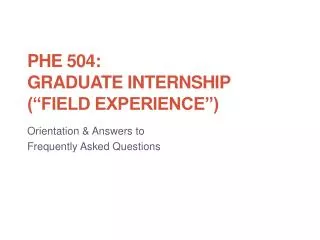
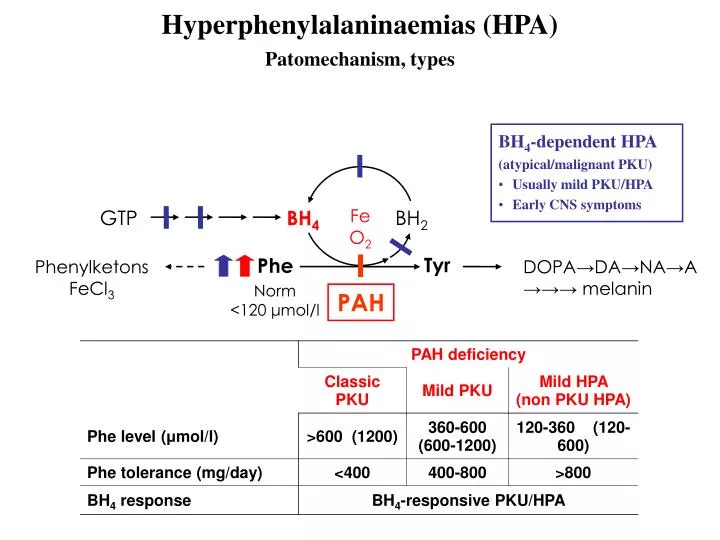
Hyperphenylalaninaemias (HPA) Patomechanism, types. BH 4 -dependent HPA (atypical/malignant PKU) Usually mild PKU/HPA Early CNS symptoms. Fe O 2. GTP. BH 4. BH 2. Tyr. Phe. Phenylketons FeCl 3. DOPA→DA→NA→A →→→ melanin. Norm <120 μ mol/l. PAH.

E N D
Hyperphenylalaninaemias (HPA) Patomechanism, types BH4-dependent HPA (atypical/malignant PKU) • Usually mild PKU/HPA • Early CNS symptoms Fe O2 GTP BH4 BH2 Tyr Phe Phenylketons FeCl3 DOPA→DA→NA→A →→→ melanin Norm <120 μmol/l PAH
0. day, screening • MS/MS (aminoacid & acylcarnitine) • Sampling on 3rd day of life • Primary parameter: blood Phe >102 μmol/l(norm < 120) Secondary parameter: Phe/Tyr > 1.5 • Clinical circumstances! • Transient hyperphenylalaninaemia • prematurity (Orn, C3 ↑) • parenteral nutrition (Val, Leu, Thr ↑ • hepatic disease (sepsis, galactosaemia,…) • drugs
Further work-up for suspected HPA newborns Positive result „normal” newborn Blood Phe 102-360 μmol/l Blood Phe >360 μmol/l Repeat screening Clinical examination week 1-3 Phe norm Phe ↑
Clinical work-up for the suspected PKU newbornsAim: definitve diagnosis, HPA typing, starting treatment • Call in the patient – no diet! • Detalied clinical history, family anamnesis • Physical examination • Usually few or no symptoms • Mild Phe elevation + feeding difficulty, hypotonia, myoclonus, seizure, salivation → atypical PKU? • Laboratory studies • Blood Phe, Phe/Tyr (MS/MS) • urine FeCl3, GC-MS • BH4 test • DNA extraction for mutation analysis • EEG
Hyperhenylalaninemia differential diagnoses BH4 test POSITIVE BH4 responsive NEGATIVE BH4 non-responsive Classic PKU / Mild HPA BH4-responsive PKU BH4-dependent (atypical) PKU
BH4 loading Phe > 360 μM normal diet diet BH4 20 mg/kg 0 4 8 12 16 24 blood Phe, Phe/Tyr (MS/MS) POSITIVE (Phe ↓ >30%) → BH4-responsive/atypical PKU? measure pterins, DHPR
Combined Phe + BH4 loading Phe < 360 μM normal diet diet Phe 100 mg/kg Phe 100 mg/kg BH4 20 mg/kg -3 0 4 8 12 16 0 4 8 12 16 24 24 -3 blood Phe, Phe/Tyr (MS/MS) POSITIVE (Phe ↓ >30%) → BH4-responsive/atypical PKU? measure pterins, DHPR
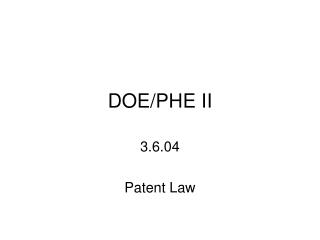
Interpreting the BH4 test result - Case 2 BH4 (20 mg/kg) Phe (100 mg/kg) 888 812 705 Phe (100 mg/kg) 122 45 40 39 1400 1200 1000 800 600 400 200 0 1193 888 Blood Phe (umol/l) BH4-dependent 387 Day 1: -3 0 4 8 12 24 hours Day 2: 24 27 31 35 39 51
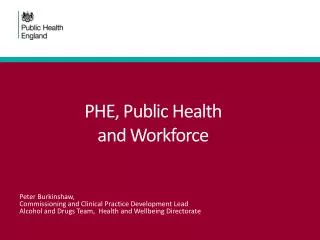
Interpreting the BH4 test result - Case 2 670 533 BH4 (20 mg/kg) 440 Phe (100 mg/kg) 254 137 96 65 42 35 1400 1200 1000 800 600 400 200 0 BH4-responsive Blood Phe (umol/l) 412 140 96 Day 1: -3 0 4 8 12 24 hours Day 2: 24 27 31 35 39 51
Molecular genetical diagnoses • Send DNA sample for mutation analysis to Semmelweis University, 2nd Dept. Pediatrics • Screen for 6 most frequent PAH mutation (R408W, R158Q, R261Q, R252W, IVS 10nt546, IVS12 splice-site) • Whole gene sequencing
Classic PKU treament, advices • Treat immediately after diagnosis • Gold standard: Phe-free medical food (enriched with vitamins, trace elements, additional energy) • Breastfeeding is encouraged, ⅓ of daily protein intakeDiet overshoot: Phe-deficiency: lethargy, feeding problem, diarrhea, anaemia, anorexia • In PKU: target Phe-level: 120-360μmol/l • In HPA (120-360 μmol/l): no treament is necessary (except pregnancy)
BH4-deficiency treament, advices • BH4 5-10 mg/kg/day • Neurotransmitter precursors: L-DOPA (Madopar 1-3, 4-7, 8-12 mg/kg/day) 5-hidroxi triptophan (Tript-OH 6-9 mg/kg/day) MAO-B blocker selegiline (0.25 mg/kg/day) • Low-Phe diet if necessary
Follow-up • Blood sample via mail regularly • Control check-ups: 0-3 years: every 3 months 3-6 years: every 6 months > 6 years: yearlyPhysical examination, laboratory studies