Download

1 / 38
380 likes | 593 Views
Alternatives to joint replacement for Knee Arthritis. Matthew Busam, MD July 17, 2008. Is there anything else you can do????. We must remember several key points… Treatment is based on symptoms, not X-rays or MRI’s No surgery is “minor surgery”

E N D
Alternatives to joint replacement for Knee Arthritis Matthew Busam, MD July 17, 2008
Is there anything else you can do???? • We must remember several key points… • Treatment is based on symptoms, not X-rays or MRI’s • No surgery is “minor surgery” • Not everything is fixed or improved with a shot or a scope • A total knee replacement is a great operation that can dramatically improve a persons quality of life.
Still, Is there anything else?? • YES. • Physical therapy • Oral medications • Supplements • Injections • Corticosteroids • Hyaluronic Acids • Arthroscopic treatments • Osteotomies
Goals • Review “arthritis” • Review therapeutic, medical, and surgical alternatives to joint replacement in the knee with arthritis.
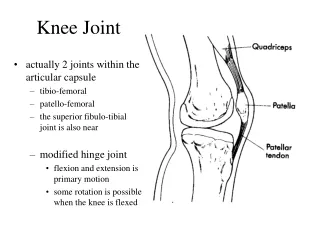
Athritis • Inflammatory or non-inflammatory degeneration of normal joint anatomy and function resulting in pain and functional disability.
Causes • Often after injury, even remote • “old trick knee” • Post surgical- total menisectomies • Obesity- • Knee joint experiences 4-8 times body weight with activity. • Genetics
Not caused by… • Sports in the absence of injury • Not even running long distances • In fact, regular exercise helps prevent joint problems • Concrete floors
General goals for patients with arthritis • Help alleviate symptoms • Allow activity • Prevent or slow progression of disease
Non-medical options • Weight loss • Losing even 10 lbs can decrease the force on an arthritic knee by 40-80 lbs! • Exercise • Strengthening the muscles around the knee can dramatically improve knee function and reduce the loads experienced by the arthritic bone.
What is a Supplement? • U.S. Food and Drug Administration (FDA) • dietary supplements: subcategory of “food,” providing manufacturers with greater leeway and less oversight than products in the pharmaceutical category • Asterisk syndrome: product is advertised to promote and maintain “joint strength,* joint flexibility,* joint lubrication,* range of motion,* production of lubricating fluid,* and renewal of cartilage and connective tissue.*” The asterisk at the bottom of the page has the following disclaimer: “*These statements have not been evaluated by the Food and Drug Administration. This product is not intended to diagnose, treat, cure, or prevent any disease.”
Supplements • “Patented ingredients help support, ease, and rebuild joints….” • “Soothe away joint pain and watch as your skin regains a nourished, youthful appearance….” • “It’s like oil for your joints—it helps promote full range of motion and flexibility.” • “New Miracle Relief Formula eliminates even the worst pain...almost instantly!”
Supplements • Glucosamine • Chondroitin • Others
Glucosamine • One meta-analysis of randomized, placebo-controlled clinical trials from January 1980 to March 2002 found glucosamine to have “highly significant efficacy” for all outcomes, including joint space narrowing and Western Ontario MacMaster University Osteoarthritis Index (WOMAC). • Structural and Symptomatic Efficacy of Glucosamine and Chondroitin in Knee Osteoarthritis A Comprehensive Meta-analysis • Florent Richy, MSc; Olivier Bruyere, MSc; Olivier Ethgen, MSc; Michel Cucherat, MSc, PhD; Yves Henrotin, MSc, PhD; Jean-Yves Reginster, MD, PhD • Arch Intern Med. 2003;163:1514-1522.
Glucosamine • Another study reported on 1,583 patients with symptomatic knee osteoarthritis who were randomly assigned to take glucosamine, chondroitin, a combination of glucosamine and chondroitin, celecoxib, or placebo over 24 weeks. Overall rate of response to glucosamine, chondroitin, and the combination were not found to be significantly better than placebo, although patients with moderate to severe pain at baseline were observed to respond significantly better with the combination. • N Engl J Med. 2006 Feb 23;354(8):795-808
Glucosamine: Side effects • Primary side effects of all salts of glucosamine are mild gastrointestinal complaints such as constipation, diarrhea, cramping, gas, heartburn, and nausea. Glucosamine sulfate has been associated with drowsiness and headache. The effects of glucosamine on nursing or pregnant women have not been well-studied. • Glucosamine may increase blood sugar levels. Although studies of glucosamine on patients with diabetes are inconclusive, it is believed that higher doses may prompt the pancreas to produce less insulin, so caution is advised. • Because glucosamine is often made from shellfish and the source of the product is not required to be on the label, individuals who are allergic to seafood are advised to exercise caution as well.
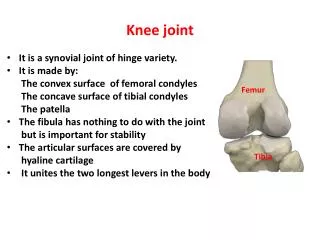
Biomechanics • Basic concept is to realign the mechanical axis to unload the arthritic compartment
Biomechanics • Mechanical axis is center of hip to center of ankle mortise • Normally just medial to tibial spines • Normal knee 60% BW through MFC
PTO Indications • Age < 60 • Single compartment involvement • 10º - 15º varus on WB x-ray • Arc of motion 90º • Flexion contracture < 15 º • Sufficient strength and motivation for rehab
PTO Contraindications • More than 20° correction • Lateral tibial subluxation > 1 cm • Medial bone loss > 2-3 mm • Severe medial/lateral ligamentous instability (varus thrust) • Inflammatory arthritis
PTO Relative Contraindications • Work comp with previous partial menisectomy • Cosmetic asymmetry • 30% over ideal body weight • Mild patellofemoral arthrosis
Medial Avoids peroneal n. and fibular osteotomy Two plane correction (slope) Technically easier Easier to revise to TKA Lateral Correct larger deformity No bone graft Known results Earlier union? Medial VS Lateral PTO
Nonunion 0-5% Malunion/ Undercorrection Patella baja 80% Infection 1-9% Peroneal palsy 5% Stiffness Lateral ligament laxity Popliteal/Ant tib artery injury DVT Intraarticular fracture Compartment syndrome AVN PTO Complications
PTO Summary • Good palliative procedure • Poor results with under- or over-correction • Results decrease at 5-10 years • Morbidity • Patella baja • Deformity • Peroneal nerve • Delayed union
Distal Femoral Osteotomy • Lateral compartment arthritis • Majority osteoarthritis • RA, neurologic (polio), collagen vascular disease, trauma • Primary DJD- 5 times more women
DFO Indications • Isolated lateral compartment arthrosis • Valgus deformity >12° or valgus joint line tilt > 10° • Arc of motion > 90° • Good rehab potential
DFO Contraindications • Rheumatoid arthritis • Tricompartmental or severe PF arthritis • Flexion contracture > 30° • Severe instability
DFO Complications • Delayed or nonunion • Malunion • Infection • Arthrofibrosis • DVT/PE • Neurovascular injury
DFO Summary • Good palliative procedure • Results appear to last longer than PTO • Less common Smaller studies
Osteochondral Allografts Results • Success ranges from 76-86% • Garrett Corr ‘94 16/17 asymtomatic at 3 years • Long term survivorship • 95% -5 year • 71% -10 years • 66% -20 years Ghavazi JBJS 1997
Osteochondral Allografts • Gross • b/t 72-92 tx’d 123 , with fresh small allografts • 5 year result 95% demonstrated successful results • results deteriorated over time with 66% successful results at 20 years Cole Ortho Spec Ed 2000
Chondrocyte Transplantation • Technique • cartilage harvested from upper medial fem condyle • sent to lab & cultured • transplanted several weeks later • periosteal flap from upper tibia obtained to cover the defect and sutured in place, sealed with fibrin glue