Download
1 / 34
740 likes | 2.25k Views
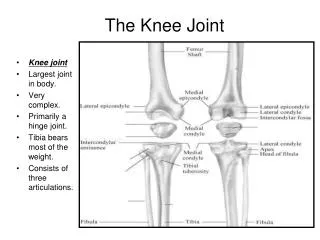
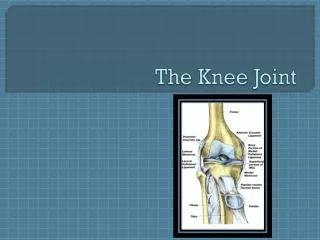
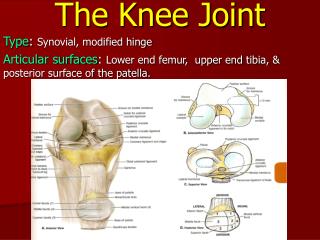
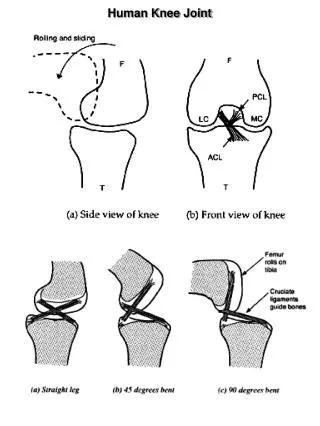
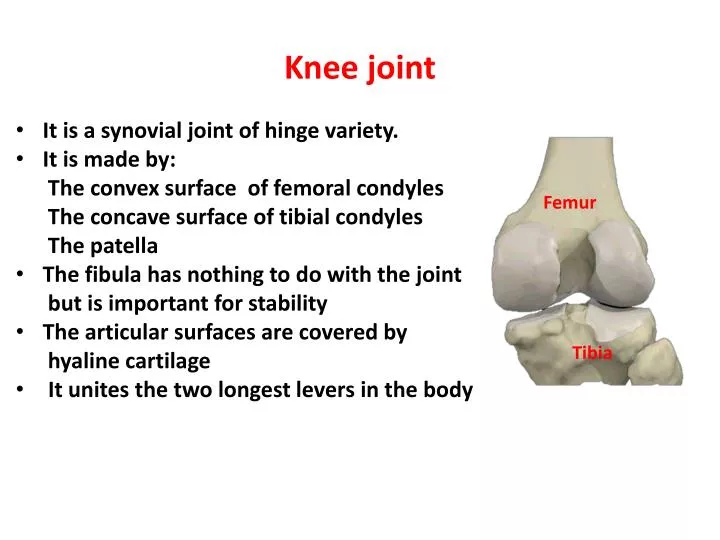
Knee joint. It is a synovial joint of hinge variety. It is made by: The convex surface of femoral condyles The concave surface of tibial condyles The patella The fibula has nothing to do with the joint but is important for stability

E N D
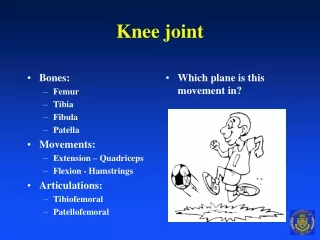
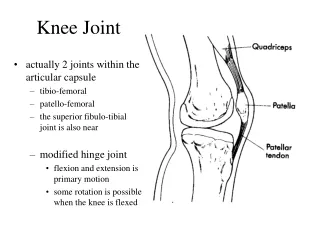
Knee joint • It is a synovial joint of hinge variety. • It is made by: The convex surface of femoral condyles The concave surface of tibial condyles The patella • The fibula has nothing to do with the joint but is important for stability • The articular surfaces are covered by hyaline cartilage • It unites the two longest levers in the body Femur Tibia
Joint Capsule • Largest in body • Surrounds entire joint, except anteriorly • A nteriorly is replaced by quadriceps tendon, patella, and patellar ligament • It is pierce by the popliteus muscle tendon
Synovial Membrane • It is intracapsular • Lines the capsule • Covers all intacapsular and extra articular surface of the joint • It also covers the cruciate ligaments • It bulges at the tendon insertions around the joint to form bursa • They minimize the friction of tendons during contraction
Bursa • 20 + associated with the knee • Most important • Subcutaneous prepatellar • Subcutaneous infrapatellar • Deep infrapatellar • Anserine bursa • Bursa deep to iliotibial band • Inferior subtendinous bursa of biceps • Popliteal bursa • Semimemranosus bursa • Gastrocnemius bursa
Extracapsular Ligaments Collateral Ligaments • Medial collateral ligament (MCL) flat band, attached above medial condyle of the femur and below to the medial surface of the shaft of the tibia – resists lateral displacement and it is weak • Lateral collateral ligament (LCL) cordlike, attached above the lateral condyle of femur and to head of the fibula below– resists medial displacement and it is strong
Extracapsular Ligaments Cont., • Oblique popliteal derived from semimembranosus on posterior aspect of the capsule, runs from that tendon to medial aspect of the lateral femoral condyle (posteriorly) • Arcuate popliteal from head of fibula, runs over the popliteus muscle to attach into posterior joint capsule • Patellar Ligament From the lower border of patella to the tibial tuberosity Oblique Popliteal Ligament Arcuate Popliteal Ligament
Intracapsular Ligaments Anterior Cruciate Ligament (ACL) • Arises from the anterior region of intercondylar area • Attached to medial side of lateral condyle • It is the weak one • It prevent hyper extension of the knee • It prevents posterior displacement of femur on tibia • It prevents anterior displacement of tibia on femur Posterior Cruciate Ligament (PCL) • Arises from the posterior region of intercondylararea • Attached to the popliteal fossa and lateral side of medial condyle • It is the strongest of the two • It prevents hyper flexion of the knee • It prevents anterior displacement of femur on tibia • It prevents posterior displacement of tibia on femur
The Menisci The articulating surface of the tibia is covered by fibrocartilaginous menisci (Medial and Lateral) Medial Meniscus: • larger than the lateral one reflects the shape of medial tibialcondyle • Anterior and posterior horns • Attached to medial collateral ligament and basically immobile Lateral Meniscus: • Smaller than medial and tighter • Almost forms a complete circle • Anterior and posterior horns • NOT attached to lateral collateral ligament
Menisci Cont., The following are involved in the attachment of the menisci to the tibial condyles • Transverse ligament anteriorly • The medial collateral ligament attaches to the medial meniscus • The tendon of semimembranosus sends fibers to the posterior edge of medial meniscus • The popliteus muscle sends fibers to the lateral meniscus • The meniscofemoral ligament extends from the lateral meniscus (post) to the inside of the medial condyle near the PCL • The coronary liagaments
Functions of Menisci • They enhance the joint stability by deepening the contact surface • They help with shock absorption by transmitting ½ of weight bearing load in full extension and some in flexion as well • They protect the articular cartilage • They transmit the load across the surface of the joint, thus reducing the load per unit area on the tibio-femoral contact sites. • The contact area in the joint is reduced 50% when the menisci are absent
Menisci Cont., • In hi load situations, 70% of the load is absorbed by the menisci, especially the lateral meniscus • The menisci assist in lubrication of the joint by acting as a space filling mechanism, more fluid is dispersed to the surface of tibia and femur • 20% increase in friction following meniscal removal
Blood Supply of the Knee Joint • Femoral Descending genicular – articular and saphenous • Popliteal Superior medial genicular, middle genicular, inferior medial genicular, superior lateral and inferior lateral genicular • Tibial Anterior and posterior tibialrecurrents • Also, anastamosis from descending branch of lateral circumflex femoral aa • Middle genicular branch sends fibers inside the joint to supply cruciate ligament, synovial membrane and periphery of menisci
Nerve Supply of the Knee Joint • According to Hilton Low, nerve supply to knee joint comes from the nerves supplying the muscles working on the knee joint. • Articular branches come from: Femoral anteriorly Tibial posteriorly Common fibular laterally Obturator and saphenous medially
Movements about the knee joint • Flexion • Extension • Internal (inward) rotation • Anterior aspect of tibia rotates inward. • External (outward) rotation • Anterior aspect of tibia rotates outward.
Movements of the Knee Joint Knee Extensors includes: • Rectus femoris (two joint muscle) • Vastusmedialis • Vastusintermedius • Vastuslateralis Knee flexors includes: • Biceps femoris (long & short) • Semimembranosus • Semitendinosus • Sartorius • Gracilis • Popliteus • Gastrocnemius Internal rotation about the knee • Popliteus • Semimembranosus • semitendinosus External rotation about the knee • biceps femoris
Muscles of the Leg The muscles are divided into the following compartments • Anterior group : • Lateral group: • Posterior group
Anterior group : Tibialis anterior: • Origin: lateral surface of tibia • Insertion: first metatarsal bone Extensor digitorumlongus: • Origin: front of fibula • Insertion: lateral four toes Extensor hallucis: • Origin: front of fibula • Insertion: big toe Peroneus tertius: • origin: front of fibula below • Insertion: fifth toe
Lateral Group Peroneus longus: • Origin: lateral side of fibula • Insertion: Plantar surface of foot medially Peroneus brevis: • Origin: lateral side of fibula • Insertion: base of 5th meta tarsal bone • Action: Eversion of the foot • Nerve supply: superficial peroneal nerve
Posterior Group Gastrocnemius: • It consists of two heads • Origin: from the lateral and medial femoral condyles Soleus: • Origin: back of tibia Plantaris: • Origin: Latera condyle of femur • All three muscles are inserted to calcaneum • Action: Plantar flextion of the foot • Nerve supply: Tibial nerve
Posterior Group Cont., • Popliteus: • Origin: Lateral condyle of femur • Insertion: back of tibia above • Action: medial rotation help in unlock the knee • Flexor hallucisLongus • Origin: back of fibula • Insertion: base of big toe • Action: Dorsiflextionof the foot • Nerve supply: Tibial nerve
Posterior Group Cont., Felxordigtorumlongus: • Origin: back of the tibia • Insertion: base of lateral four toes Tibialisposterior: • Origin: Back of tibia • Insertion:Base of metatarsal bones • Action of both muscles: Dorsiflextion of the foot • Nerve supply: Tibial nerve
Tibialis Anterior Extensor Hallucis extensorDigitorum Tibialis Posterior Peroneus Longus Peroneus Brevis Flexor Digitorum Flexor Hallucis Soleus Plantaris Gastrocnemius L Gastrocnemius M
Blood Supply of the leg • Popliteal artery is the continuation of femoral artery at adductor hiatus • Gives: Anterior tibial artery Posterior tibial which gives the peroneal artery
Q angle • An angle found by drawing a line from ASIS to middle of patella and a second line from mid patella to tibialtuberosity • Represents efficiency of Quadreceps • Most efficient = 10 degree • Males range from 10-14 degree • Females from 15-17 degree • Represents the valgus stress acting on knee • Great than 17 called genu Valgum or knock knees • Very small angle causes gen varum
Knee deformities Genu valgus Genu varus
Applied anatomy • Fracture tibia (subcutaneous) x-rays
Applied anatomy • Prone to injury (sports) • Med. Meniscus } • Med. Coll. Lig. }unhappy triad • Ant. Cruciate } • Swelling (synovial cavity and bursa) • Pre-patella bursitis (“housemaids knee”) • Osteoarthritis and knee replacement • Deformities • Valgus and varus • Recurrent dislocation of patella (females)
Movement and stability • Movements are flexion & extension • Medial & lateral rotation (lock & unlock) • A stable joint due to strong muscles and ligaments
Support of the Joint • Knee supports the weight of the body and transmits forces from the ground • Functional stability of the joint is derived from the passive restraint of the ligaments, the active support of muscles, the joint geometry, and the compressive forces pushing the bones together