Download
1 / 36
510 likes | 1.55k Views
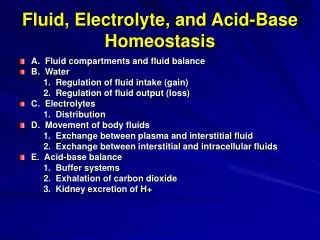
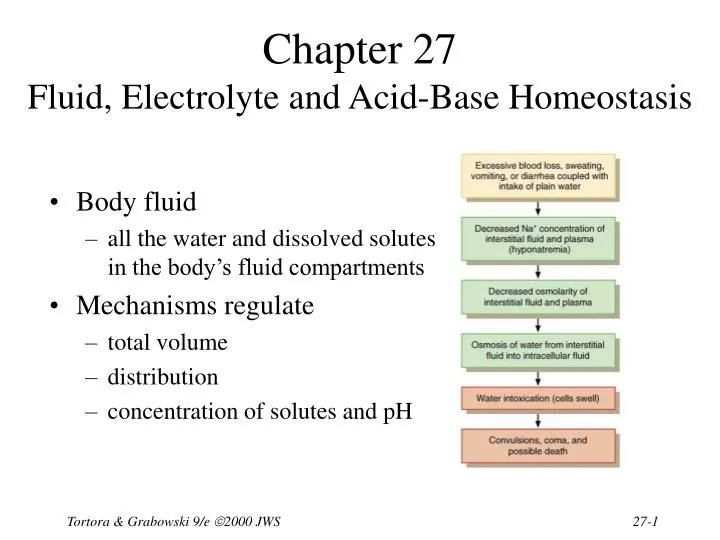
Chapter 27 Fluid, Electrolyte and Acid-Base Homeostasis. Body fluid all the water and dissolved solutes in the body’s fluid compartments Mechanisms regulate total volume distribution concentration of solutes and pH. Balance Between Fluid Compartments.

E N D
Chapter 27Fluid, Electrolyte and Acid-Base Homeostasis • Body fluid • all the water and dissolved solutes in the body’s fluid compartments • Mechanisms regulate • total volume • distribution • concentration of solutes and pH Tortora & Grabowski 9/e 2000 JWS
Balance Between Fluid Compartments Volume of fluid in each is kept constant. Since water follows electrolytes, they must be in balance as well • Only 2 places for exchange between compartments: • cell membranes separate intracellular from interstitial fluid. • only in capillaries are walls thin enough for exchange between plasma and interstitial fluids Tortora & Grabowski 9/e 2000 JWS
Body Water Gain and Loss • 45-75% body weight • declines with age since fat contains almost no water • Gain from ingestion and metabolic water formed during aerobic respiration & dehydration synthesis reactions (2500 mL/day) • Normally loss = gain • urine, feces, sweat, breathe Tortora & Grabowski 9/e 2000 JWS
Regulation of Water Gain • Formation of metabolic water is not regulated • function of the need for ATP • Main regulator of water gain is intake regulation • Stimulators of thirst center in hypothalamus • dry mouth, osmoreceptors in hypothalamus, decreased blood volume causes drop in BP & angiotensin II • Drinking occurs • body water levels return to normal Tortora & Grabowski 9/e 2000 JWS
Dehydration Stimulates Thirst • Regulation of fluid gain is by regulation of thirst. Tortora & Grabowski 9/e 2000 JWS
Regulation of Water and Solute Loss • Elimination of excess water or solutes occurs through urination • Consumption of very salty meal demonstrates function of three hormones • Demonstrates how • “water follows salt” • excrete Na+ and water will follow and decrease blood volume Tortora & Grabowski 9/e 2000 JWS
Hormone Effects on Solutes • Angiotensin II and aldosterone promote reabsorption of Na+ and Cl- and an increase in fluid volume • stretches atrial volume and promotes release of ANP • slows release of renin & formation of angiotensin II • increases filtration rate & reduces water & Na+ reabsorption • decreases secretion of aldosterone slowing reabsorption of Na+ and Cl- in collecting ducts • ANP promotes natriuresis or the increased excretion of Na+ and Cl- which decreases blood volume Tortora & Grabowski 9/e 2000 JWS
Hormone Regulation of Water Balance • Antidiuretic hormone (ADH) from the posterior pituitary • stimulates thirst • increases permeability of principal cells of collecting ducts to assist in water reabsorption • very concentrated urine is formed • ADH secretion shuts off after the intake of water • ADH secretion is increased • large decrease in blood volume • severe dehydration and drop in blood pressure • vomiting, diarrhea, heavy sweating or burns Tortora & Grabowski 9/e 2000 JWS
Movement of Water • Intracellular and interstitial fluidsnormally have the same osmolarity,so cells neither swell nor shrink • Swollen cells of water intoxicationbecause Na+ concentration of plasmafalls below normal • drink plain water faster than kidneys canexcrete it • replace water lost from diarrhea or vomitingwith plain water • may cause convulsions, coma & death unless oral rehydration includes small amount salt in water intake Tortora & Grabowski 9/e 2000 JWS
Enemas and Fluid Balance • Introduction of a solution into the bowel to stimulate activity and evacuate feces • Increase risk of fluid & electrolyte imbalance unless isotonic solution is used Tortora & Grabowski 9/e 2000 JWS
Concentrations of Electrolytes • Functions of electrolytes • control osmosis between fluid compartments • help maintain acid-base balance • carry electric current • cofactors needed for enzymatic activity • Concentration expressed in mEq/liter or milliequivalents per liter for plasma, interstitial fluid and intracellular fluid Tortora & Grabowski 9/e 2000 JWS
Comparison Between Fluid Components • Plasma contains many proteins, but interstitial fluid does not • producing blood colloid osmotic pressure • Extracellular fluid contains Na+ and Cl- • Intracellular fluid contains K+ and phosphates (HPO4-2) Tortora & Grabowski 9/e 2000 JWS
Sodium • Most abundant extracellular ion • accounts for 1/2 of osmolarity of ECF • Average daily intake exceeds normal requirements • Hormonal controls • aldosterone causes increased reabsorption Na+ • ADH release ceases if Na+ levels too low--dilute urine lost until Na+ levels rise • ANP increases Na+ and water excretion if Na+ levels too high Tortora & Grabowski 9/e 2000 JWS
Edema, Hypovolemia and Na+ Imbalance • Sodium retention causes water retention • edema is abnormal accumulation of interstitial fluid • Causes of sodium retention • renal failure • hyperaldosterone • Excessive loss of sodium causes excessive loss of water (low blood volume) • due to inadequate secretion of aldosterone • too many diuretics Tortora & Grabowski 9/e 2000 JWS
Chloride • Most prevalent extracellular anion • Moves easily between compartments due to Cl- leakage channels • Helps balance anions in different compartments • Regulation • passively follows Na+ so it is regulated indirectly by aldosterone levels • ADH helps regulate Cl- in body fluids because it controls water loss in urine • Chloride shift & hydrochloric acid of gastric juice Tortora & Grabowski 9/e 2000 JWS
Potassium • Most abundant cation in intracellular fluid • Helps establish resting membrane potential & repolarize nerve & muscle tissue • Exchanged for H+ to help regulate pH in intracellular fluid • Control is mainly by aldosterone which stimulates principal cells to increase K+ secretion into the urine • abnormal plasma K+ levels adversely affect cardiac and neuromuscular function Tortora & Grabowski 9/e 2000 JWS
Bicarbonate • Common extracellular anion • Major buffer in plasma • Concentration increases as blood flows through systemic capillaries due to CO2 released from metabolically active cells • Concentration decreases as blood flows through pulmonary capillaries and CO2 is exhaled • Kidneys are main regulator of plasma levels • intercalated cells form more if levels are too low • excrete excess in the urine Tortora & Grabowski 9/e 2000 JWS
Calcium • Most abundant mineral in body (skeleton & teeth) • Abundant extracellular cation in body fluids • Important role in blood clotting, neurotransmitter release, muscle tone & nerve and muscle function • Regulated by parathyroid hormone • stimulates osteoclasts to release calcium from bone • increases production of calcitriol (Ca+2 absorption from GI tract and reabsorption from glomerular filtrate) Tortora & Grabowski 9/e 2000 JWS
Phosphate • Present as calcium phosphate in bones and teeth, and in phospholipids, ATP, DNA and RNA • HPO4-2 is important intracellular anion and acts as buffer of H+ in body fluids and in urine • mono and dihydrogen phosphate act as buffers in the blood • Plasma levels are regulated by parathyroid hormone & calcitriol • resorption of bone releases phosphate • in the kidney, PTH increase phosphate excretion • calcitriol increases GI absorption of phosphate Tortora & Grabowski 9/e 2000 JWS
Magnesium • Found in bone matrix and as ions in body fluids • intracellular cofactor for metabolic enzymes, heart, muscle & nerve function • Urinary excretion increased in hypercalcemia, hypermagnesemia, increased extracellular fluid volume, decreases in parathyroid hormone and acidosis Tortora & Grabowski 9/e 2000 JWS
Acid-Base Balance • Homeostasis of H+ concentration is vital • proteins 3-D structure sensitive to pH changes • normal plasma pH must be maintained between 7.35 - 7.45 • diet high in proteins tends to acidify the blood • 3 major mechanisms to regulate pH • buffer system • exhalation of CO2 (respiratory system) • kidney excretion of H+ (urinary system) Tortora & Grabowski 9/e 2000 JWS
Actions of Buffer Systems • Prevent rapid, drastic changes in pH • Change either strong acid or base into weaker one • Work in fractions of a second • Found in fluids of the body • 3 principal buffer systems • protein buffer system • carbonic acid-bicarbonate buffer system • phosphate buffer system Tortora & Grabowski 9/e 2000 JWS
Protein Buffer System • Abundant in intracellular fluids & in plasma • hemoglobin very good at buffering H+ in RBCs • albumin is main plasma protein buffer • Amino acids contains at least one carboxyl group (-COOH) and at least one amino group (-NH2) • carboxyl group acts like an acid & releases H+ • amino group acts like a base & combines with H+ • some side chains can buffer H+ • Hemoglobin acts as a buffer in blood by picking up CO2 or H+ Tortora & Grabowski 9/e 2000 JWS
Carbonic Acid-Bicarbonate Buffer System • Acts as extracellular & intracellular buffer system • bicarbonate ion (HCO3-) can act as a weak base • holds excess H+ • carbonic acid (H2CO3) can act as weak acid • dissociates into H+ ions • At a pH of 7.4, bicarbonate ion concentration is about 20 times that of carbonic acid • Can not protect against pH changes due to respiratory problems Tortora & Grabowski 9/e 2000 JWS
Phosphate Buffer System • Most important intracellularly, but also acts to buffer acids in the urine • Dihydrogen phosphate ion acts as a weak acid that can buffer a strong base • Monohydrogen phosphate acts a weak base by buffering the H+ released by a strong acid Tortora & Grabowski 9/e 2000 JWS
Exhalation of Carbon Dioxide • Breathing plays a role in the homeostasis of pH • pH modified by changing rate & depth of breathing • faster breathing rate, blood pH rises • slow breathing rate, blood pH drops • H+ detected by chemoreceptors in medulla oblongata, carotid & aortic bodies • Respiratory centers inhibited or stimulated by changes is pH Tortora & Grabowski 9/e 2000 JWS
Kidney Excretion of H+ • Metabolic reactions produce 1mEq/liter of nonvolatile acid for every kilogram of body weight • Excretion of H+ in the urine is only way to eliminate huge excess • Kidneys synthesize new bicarbonate and save filtered bicarbonate • Renal failure can cause death rapidly due to its role in pH balance Tortora & Grabowski 9/e 2000 JWS
Acid-Base Imbalances • Acidosis---blood pH below 7.35 • Alkalosis---blood pH above 7.45 • Compensation is an attempt to correct the problem • respiratory compensation • renal compensation • Acidosis causes depression of CNS---coma • Alkalosis causes excitability of nervous tissue---spasms, convulsions & death Tortora & Grabowski 9/e 2000 JWS
Summary of Causes • Respiratory acidosis & alkalosis are disorders involving changes in partial pressure of CO2 in blood • Metabolic acidosis & alkalosis are disorders due to changes in bicarbonate ion concentration in blood Tortora & Grabowski 9/e 2000 JWS
Respiratory Acidosis • Cause is elevation of pCO2 of blood • Due to lack of removal of CO2 from blood • emphysema, pulmonary edema, injury to the brainstem & respiratory centers • Treatment • IV administration of bicarbonate (HCO3-) • ventilation therapy to increase exhalation of CO2 Tortora & Grabowski 9/e 2000 JWS
Respiratory Alkalosis • Arterial blood pCO2 is too low • Hyperventilation caused by high altitude, pulmonary disease, stroke, anxiety, aspirin overdose • Renal compensation involves decrease in excretion of H+ and increase reabsorption of bicarbonate • Treatment • breathe into a paper bag Tortora & Grabowski 9/e 2000 JWS
Metabolic Acidosis • Blood bicarbonate ion concentration too low • loss of ion through diarrhea or kidney dysfunction • accumulation of acid (ketosis with dieting/diabetes) • kidney failing to remove H+ from protein metabolism • Respiratory compensation by hyperventilation • Treatment • IV administration of sodium bicarbonate • correct the cause Tortora & Grabowski 9/e 2000 JWS
Metabolic Alkalosis • Blood bicarbonate levels are too high • Cause is nonrespiratory loss of acid • vomiting, gastric suctioning, use of diuretics, dehydration, excessive intake of alkaline drugs • Respiratory compensation is hypoventilation • Treatment • fluid and electrolyte therapy • correct the cause Tortora & Grabowski 9/e 2000 JWS
Diagnosis of Acid-Base Imbalances • Evaluate • systemic arterial blood pH • concentration of bicarbonate (too low or too high) • PCO2 (too low or too high) • Solutions • if problem is respiratory, the pCO2 will not be normal • if problem is metabolic, the bicarbonate level will not be normal Tortora & Grabowski 9/e 2000 JWS
Homeostasis in Infants • More body water in ECF so more easily disrupted • Rate of fluid intake/output is 7X higher • Higher metabolic rate produces more metabolic wastes • Kidneys can not concentrate urine nor remove excess H+ • Surface area to volume ratio is greater so lose more water through skin • Higher breathing rate increase water loss from lungs • Higher K+ and Cl- concentrations than adults Tortora & Grabowski 9/e 2000 JWS
Impaired Homeostasis in the Elderly • Decreased volume of intracellular fluid • inadequate fluid intake • Decreased total body K+ due to loss of muscle tissue or potassium-depleting diuretics for treatment of hypertension or heart disease • Decreased respiratory & renal function • slowing of exhalation of CO2 • decreased blood flow & glomerular filtration rate • reduced sensitivity to ADH & impaired ability to produce dilute urine • renal tubule cells produce less ammonia to combine with H+ and excrete as NH+4 Tortora & Grabowski 9/e 2000 JWS