Download
1 / 99
1.13k likes | 1.66k Views
Cardiovascular Pathology (modification of Dr. Veinot’s presentation). Michel Dionne MD FRCPC for John P. Veinot MD FRCPC Professor of Pathology University of Ottawa Pathology and Laboratory Medicine Ottawa Hospital.

E N D
Cardiovascular Pathology(modification of Dr. Veinot’s presentation) Michel Dionne MD FRCPC for John P. Veinot MD FRCPC Professor of Pathology University of Ottawa Pathology and Laboratory Medicine Ottawa Hospital
You may only access and use this PowerPoint presentation for educational purposes. You may not post this presentation online or distribute it without the permission of the author.
Overview Atherosclerosis Aneurysms Ischemic heart disease Cardiomyopathies Valvular heart disease Hypertension
muscular artery intima media adventitia
Atherosclerosis Disease of large and medium sized arteries (elastic and muscular), particularly: aorta, iliac, coronary, popliteal, carotid, circle of Willis Develop intimal lesions called atheromas or atheromatous plaques which: protrude into the lumen resulting in stenosis (narrowing of lumen) and possibly occlusion (lumen blocked) can weaken the underlying media, possibly leading to aneurysm formation
Atherosclerosis - risk factors Hyperlipidemia high LDL low HDL Hypertension Smoking Diabetes Age Male gender Family history/ genetics Other: physical inactivity, diet, obesity etc.
Atherosclerosis - pathogenesis • Chronic endothelial injury* resulting in endothelial dysfunction • increased permeability • increased adhesion of leukocytes (monocytes and lymphocytes) and platelets • accumulation of lipids in intima • Migration of monocytes into intima leading to formation of foam cells (lipid-laden macrophages) • Release of cytokines and growth factors result in smooth muscle cell migration into intima, proliferation of smooth muscle cells, deposition of extracellular matrix (e.g. collagen) * From hemodynamic forces, hyperlipidemia, HTN, smoking etc.
From: Robbins and Cotran Pathologic Basis of Disease, 8th Edition
Aortic arch vessels – advanced plaques causing severe stenosis
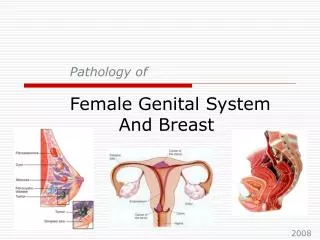
Atheromatous material – foam cells (lipid laden macrophages) and cholesterol clefts
From: Robbins and Cotran Pathologic Basis of Disease, 8th Edition
Atherosclerosis - complications Calcification Plaque hemorrhage and rupture Plaque erosion/ulceration Thrombosis Embolization of atheromatous material (atheroemboli) Aneurysm formation and rupture
Atherosclerosis - major consequences Symptomatic disease most often affects the heart, brain, kidneys and lower extremities Heart: angina and myocardial infarction Brain: cerebral infarction (stroke) Aorta (particularly abdominal): Aneurysms Stenosis of ostia of major branches leading to visceral ischemia Lower extremities: peripheral vascular (arterial) disease – claudication, gangrene
Aneurysm - definition a localized abnormal dilatation of a vessel
Aneurysm types Atherosclerotic aneurysms are the most common, but there are other types!
Aneurysms - complications Stasis of blood Thrombosis obstruction embolism Mass effect Rupture
Abdominal Aortic Aneurysm (AAA) thrombus
Aneurysm rupture blood lumen tear thrombus vessel wall
AAA rupture Hemorrhage into surrounding tissue
Coronary artery aneurysms secondary to vasculitis (inflammation of blood vessels)
Left lung SVC Aorta Left atrium Pericardium Right lung Right atrium Left ventricle Right ventricle
Left atrium Right atrium Left ventricle Right ventricle Interventricular septum
Coronary artery anatomy http://www.drchander.com/diagnoseCAD.html
Coronary artery atherosclerosis affects the epicardial arteries; tends to be more pronounced in the proximal portion of these vessels can involve 1, 2 or all 3 of the main vessels +/- their large branches if degree of obstruction is significant, can result in angina (pain from myocardial ischemia) an atherosclerotic plaque can become unstable (acute plaque lesion): intraplaque hemorrhage plaque rupture or erosion resulting in thrombosis acute plaque lesions can result in an “acute coronary syndrome” (unstable angina, myocardial infarct)
Recent MI - 7-10 days old “Sick” myocytes bordering the infarct Phagocytosis of dead cells at margin of infarct Residual necrotic myocytes