Download
1 / 19
280 likes | 762 Views
P-glycoproteins. Jessica R Oesterheld, MD. MDR1->P-gps. 27 years ago, Juliano and Ling noted after initial efficacy, many anti-CA drugs stopped being effective at the same time= Multiple Drug Resistance (MDR)

E N D
P-glycoproteins Jessica R Oesterheld, MD
MDR1->P-gps • 27 years ago, Juliano and Ling noted after initial efficacy, many anti-CA drugs stopped being effective at the same time= Multiple Drug Resistance (MDR) • The gene MDR1 on chromosome 7 encodes a glycoprotein named P (permeability) glycoprotein that actively pumps out compounds from cell • Multiple drugs are effected at same time since ALL are P-gp substrates
Pgp is on the apical surface of endothelial cells lining the brain capillaries that forms BBB (From David Flockhart)
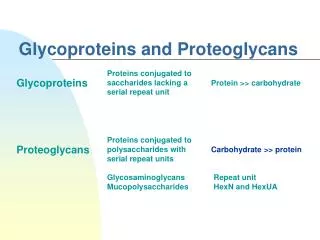
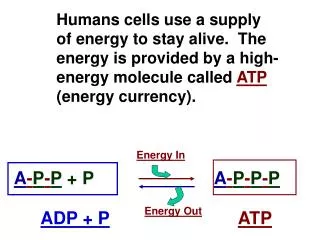
P-gps • A member of a large family of “transporters” that use ATP (ATP-Binding Cassette transporters= ABC transporters)to flip compounds across a cellular gradient= “flippases” or “bouncers”or “hydrophobic vaccuum cleaners” • Classification:http://nutrigene.4t.com/humanabc.htm since October 1999 • More than 45 transporters; divided into 7 subfamilies • Different transporters effect glucuronides, organic anions etc • Pgp-1=PGY1 (ABCB1) in MDR subfamily
Limits cell uptake and extrudes drugs • P-gps exist in membranes of tumor cells and in liver, bile duct, kidneys, placenta, BBB, luminal cells of jejunum, heart • BBB, testes, placenta, P-gps blocks entry of compounds into these “sanctuaries” • In kidney, liver and small intestine, P-gps efflux compounds into the gut lumen, bile, urine
Some drugs are P-gp substrates • Drugs can be P-gp substrates or not (see list for P-gp substrates) • Older antihistamines are not P-gp substrates therefore they enter the BBB, but non-sedating antihistamines are P-gp substrates and are excluded from the CNS and have less CNS side effects
Some drugs are P-gp inhibitors/inducers • New kind of drug-drug interaction • Usually anti-diarrheal drug loperamide is excluded by BBB from CNS because it is a P-gp substrate. If add quinidine which is a P-gp inhibitor at sufficient dosage, patient will get CNS side effect or respiratory depression (Sadeque and Wandel 2000)
Some drugs are P-gp inhibitors/inducers-2 • Long known that quinidine given with digoxin-> increased digoxin concentration • Only a small portion of digoxin is handled by CYPs, but digoxin is a P-gp substrate • Quinidine blocks P-gp in kidney, more digoxin is retained
Variabilities in amount of P-gps 8-fold variation in gut in renal transplant patients (Lown et al 1997); 4-fold in nonmedicated adults (Johnson 2002) • Controversial whether men have 2 fold higher levels of P-gps than women • C3435T in exon 26 TT (mutant) associated with lower intestinal P-gp activity and 2-fold higher dig concentrations since not a CYP3A substrate, less kicked into lumen (Hoffmeyer et al 2000,) and increased frequency of nortriptyline- induced postural hypotension, (Roberts et al 2002) **in a non-coding, non-promoting position and is probably linked to another region=surrogate
Variabilities-amount of P-gps-2 • C3435T in exon 26 CC (associated with higher P-gp activity)- and anti-seizure medication resistance (Siddiqui et al 2003)
Variabilities in P-gps • In gut, more P-gp protects against gastroenteritis in tropics---natural selection breeds those with higher amounts • wild type (cc) 83% Ghanians 61% African-Americans 26% Whites (Schaeffeler et al 2001) -to get similar blood levels of tacrolimus or cyclosporin in African Americans, need higher dosing as compared to causasians
Intestinal Cells drug pgp 3A4 drug LUMEN pgp 3A4 drug pgp 3A4 P-gps in “front”- with repeated shuttles of absorption/efflux
Intestinal P-gps (Lin and Yamazaki 2003) • Misconception that if a drug is a P-gp substrate, then it has low bioavailability • Amount of drug absorbed = influx (passive diffusion + active uptake) - efflux (P-gp +amount metabolized by CYPs +Phase 2) • P-gp functional activity is saturable, therefore when drug at low dose or poor permeability, P-gp effect more important
CYP3A and P-gps work together in the gut • Many substrates of P-gps are also CYP3A4 substrates • In small intestine, P-gps efflux compound to lumen, then compound is reabsorbed; this “shuttle” leads to increased “exposure” of compounds to CYP3A4 and maximizes their activity
Double Inhibitors/Double Inducers in the gut • Many drugs are both P-gp and CYP3A4 inhibitors (e.g., gfj, erythromycin, cyclosporin) • Many drugs are both P-gp and CYP3A4 inducers (e.g., St Johns wort, rifampin) • DDIs related to CYPs or P-gps or both • Coordination - PXR and perhaps other mechanisms
Pgp knockout mice Pgp knockout mice show increased sensitivity to ivermectin since it can now cross BBB (Smit et al 1999) • Also digoxin, cyclosporin, vinblastine colchicine • But if give cyclosporin (Pgp inh) before you give ivermectin->brain conc 2.5 times higher (Margues-Santos 1999) • Induce first with dexamethasone or morphine--> decreased brain concentration of Pgp substrates
Clinical use of P-gp Inhibitors • Cli nical use of P-gp inhibitors to block development of MDR in pts with Ca have no absolute success despite 15 yrs of trying • 3 generations 1-cyclosporin -intrinsic toxicity 2- valsopodar -analog devoid of intrinsic toxicity 3- tariquidar • 3rd gen drugs are not CYP3A4 inhibitors or other transporter inhibitors, very potent, and perhaps effect ATP
Very difficult to predict P-gp DDIs • Not a simple docking station • At least 2 binding sites and 2 ATP-binding sites on 2 symmetric non-identical halves of P-gp • Sites work cooperatively • Competitive inhibition, non-competitive inhibition and collective stimulation • Substrate specific • Must also tease out CYP3A4 effects and other transporters • Important with digoxin, cyclosporin