Download
1 / 52
560 likes | 997 Views
Peptic Ulcer Disease. Epidemiology. Occurs in 5-10% of US population Multiple causes include infection (h. pylori), drugs (NSAID), and chemical (XS acid). Primary ulceration on the decline however drug-induced incidence is increasing due to increased use of NSAIDs. Physiology.

E N D
Epidemiology Occurs in 5-10% of US population Multiple causes include infection (h. pylori), drugs (NSAID), and chemical (XS acid). Primary ulceration on the decline however drug-induced incidence is increasing due to increased use of NSAIDs.
Physiology Acid secretion Mucosal defense barrier
k Somatostatin k Physiology: Acid Secretion The parietal cell and gastric acid secretion
Physiology: Acid Secretion Stimulation of acid secretion
Pathophysiology Summary of pathogenic mechanisms in ulcer disease
Pathophysiology Acid & Gastrin levels vary in gastric and Duodenal Ulcer Same relationship for basal and peak levels of acid & gastrin
Pathophysiology Primary association with H. pylori
Pathophysiology: H. pylori • H. pylori promotes ulceration by: • 1. inducing local inflammation and damage to the mucosal barrier. • 2. removing feedback inhibition of acid secretion.
Pathophysiology: H. pylori Gastric metaplasia
Pathophysiology: H. pylori Helicobacter pylori's initiation of mucosal inflammation leads to loss of protective mechanisms of gastric mucosa.
Pathophysiology: H. pylori Acid Gastrin
H. pylori: 2005 Nobel Prize in Physiology & Medicine
Pathophysiology: NSAID induced ulcer
NSAID induced ulcer Physiology of endogenous prostaglandins in the stomach: 1. PGE2 and PGI2 synthesized in the gastric mucosa by COX-1 inhibit acid production by binding the EP3 receptor on parietal cells (endogenous regulation of cAMP). 2. PGE2 prevents gastric injury by stimulating the secretion of mucous and bicarbonate in superficial epithelial cells, and by increasing mucosal blood flow. NSAID-Induced Injury: 1. NSAIDs block cyclooxygenase-1 (COX-1). 2. Systemic and localized inhibition of COX-1 can: a. Decrease endogenous regulation of gastric acid release, resulting in higher basal gastric acid levels between meals. b. Decrease bicarbonate and mucous production, resulting in the loss of mucosal integrity. 3. Aspirin and many NSAIDs can directly injure or irritate the stomach lining.
Pathophysiology: Zollinger-Ellison ZE Syndrome Less common (~ 1%) Chemical-induced PUD
Pathophysiology: ZE Gastrin staining of duodenal gastrinoma
Pathophysiology: ZE Location of gastrinomas
Pathophysiology: ZE -Gastrin secretion is unregulated -Gastrin and Acid levels extremely high -20% cases are MEN I -no H. pylori present & no use of NASIDs
Pathophysiology: ZE Gastric folds in patient with ZE syndrome
Clinical Features Clinical manifestations of ulcer disease
Clinical Features Complications Bleeding in 10-80%
Clinical Features Complications Recurrent bleeding
Clinical Features Complications: Peptic ulcer perforation
Clinical Features Complications: Outflow Obstruction Acute: inflammation & muscle spasm Chronic: fibrosis & scar formation
Clinical Features Cigarette smoking on ulcer recurrence
Diagnosis Radiographic features of gastric ulcer
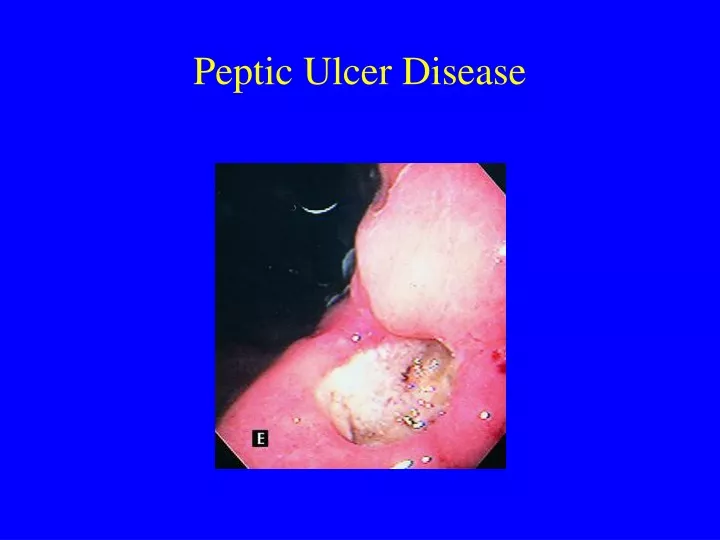
Diagnosis Endoscopy: duodenal ulcer
Diagnosis Endoscopy: gastric ulcer
Diagnosis Urea breath test
Treatment: based on pathology & physiology Summary of pathogenic mechanisms in ulcer disease
k Somatostatin k Treatment: H-2 receptor Antagonists Plus H2 blocker
Treatment: Proton Pump Inhibitor (PPI) (n.b.: binding of PPIs is irreversible)
Treatment: Proton Pump Inhibitor (PPI) Degree of acid suppression and rate of duodenal ulcer healing
Triple Therapy: Bismith, metronizadole, plus amoxicillin or tetracycline
Treatment: Duodenal ulcer healing with Helicobacter pylori treatment + H2 blockers
Treatment: PPIs, but not antibiotics, have added benefit of reducing GERD .