Download
1 / 47
470 likes | 731 Views
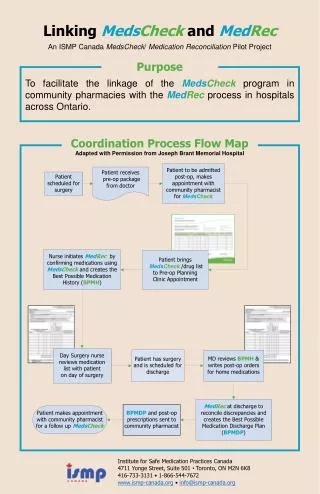
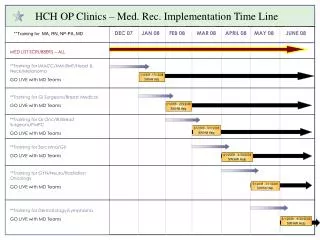
Pharmacy's Role in Improving Patient Care - Moving from Med WRECK to Med Rec. Bruce Thompson, RPh, M.S. Hennepin County Medical Center. Learning Objectives . At the conclusion of the program, the participant will learn:

E N D
Pharmacy's Role in Improving Patient Care - Moving from Med WRECK to Med Rec Bruce Thompson, RPh, M.S. Hennepin County Medical Center
Learning Objectives At the conclusion of the program, the participant will learn: Identify steps to consider reducing patient readmission from a pharmacy perspective Understand the barriers with medication discharge process Adopt a process to develop new services
First Project Medication Error on Discharge. Medication Not continued Medication restarted that should not
Pilot First 30 patients, only 8 % were Error Free
Pilot Added Pharmacists to review Discharge Medication Orders 129 Patients average over 6 months
Pilot Step one, Improvements in EPIC Still 70% had potential Errors
Pilot Improved Process and Pharmacists improved Readmission Rate by 47% !
Pilot Reduced from 10.2 % to 5.4% Now after 15 months still below 6%.
Pilot Added Pharmacists to provide service for all Patients in this category. Slowly Expanded to other high risk areas
Next Phase CCDS – Coordinated Care Delivery System
Patient Stratification: A blueprint for Reducing Readmissions
Tier I Care ZL 53 YO woman transfers to HCMC CCDS Six chronic medical problems (includes DMII) only four meds Complex social issues (joblessness, social isolation, home foreclosure with homelessness) May 2010 Inpatient Psych admit with suicidality Disrupted a multi-year primary care provider relationship Requesting primary care and mental health follow-up Meeting mental health needs a challenge
Tier II Care JL 62 YO woman severe alcoholism Heart and nerve toxicity, back pain Independent but vulnerable Admitted 6/17- 6/20 – Failure to thrive Readmission 6/29-7/3 – Cognition assessed, chemical dependency treatment refused Successful Primary Care follow up 6 days after discharge Medication simplification, contact with home RN Now lost to follow up
Tier III Care JF 37 YO homeless man Asthma, recent pulmonary embolism Schizoaffective D/O – likely Cocaine abuse – certain Chronic abdominal pain from pancreatitis – possible Nominally involved in chemical dependency treatment Spring 2010 – 6 admits with $225,000 in charges
23 Percent of patients with over 10 active medications Tier I. 46 Percent in Tier II and Tier III have over 10 medications.
Tier III care Coordinated Care Center opened mid-July 100/300 patients assigned Predominately from inpatient care Multi-disciplinary team: MDs, NPs, Pharmacist, Social Worker, Care Managers, chemical dependency counselor and Mental health member.
Tier III care Intensive medical care and multi-disciplinary care Low visit volume, high contact/management model Expensive: 4-5 professional FTEs/150 patients Twice weekly care team meetings
Reduction in Readmissions Readmission rate reduced by 30-50% Total Hospitalizations reduced by 43%. ER Visits reduced by 37%
Pharmacy Role in Reducing Readmissions Medication Reconciliation Both Admission and Discharge Right Medication Medication Therapy Management Visits within 5 days of discharge Routine appointments based on patients Automatic Refills Deliver to Clinics, Provider or MTM
Med Rec Proven Success with a program that documented a reduction in readmissions by 47%. Value realized by Providers
MTM Services Proven Track record with Clinics Visits increased in past 18 months. Increased Revenue. Improved Care Decrease total Health Care expenses
RX Delivery Adapt process for CCDS Clinic Auto refill medications Deliver to clinics to avoid long waits MTM Pharmacists improve patient compliance.
Administrative Approval Pharmacy are integral to the success of the program!
Additional Pilots Projects Similar results with Psychiatry and Medicine
Where do we go from here? • Get involved with Care Redesign. • Propose MTM services • Evaluate Accuracy of Discharge Medications. • Need Community Pharmacies to work with your health care system.
Health-System Pharmacy and Care Transitions Moving from DRG/RVU to ACO Craig Else, PharmD, MHA Fairview Health System
Care Transition Models • Eric Coleman (www.caretransitions.org) • Four Pillars • Medication Self-Management • Dynamic Patient-Centered Record • Follow-up • Red Flags
Care Transitions Models (cont’d) • Project RED (Re-Engineered Discharge) • 8 similar points • Louise videos • https://www.bu.edu/fammed/projectred/index.html • BOOST (Better Outcomes for Older Adults through Safe Transitions) • 9P Criteria (Problem Meds, Psych, Polypharmacy, Diagnosis, Health Literacy, Readmissions, Support, Palliative Care) • http://www.hospitalmedicine.org
Care TransitionsGoals • Decreased Readmissions • Lower Total Cost of Care • Increased Patient Satisfaction • Increased Clinical Quality Triple Aim!
Fairview’s Transition Projects • carol.com/Fairview Ridges • UMMC Pediatrics • FPA/Ucare/Fairview Southdale • MTM/CHF • MTM/Eagan Clinic
Fairview Ridges • Facilitated by carol.com • CHF/COPD patients • Pharmacy Discharge Reconciliation and Education • Home Care follow up • MTM follow up
Advantages/Disadvantages • Want list to be clear, but complete • Pictures can be problematic • Add/Change/Discontinue section • Times? • Indication? • MD? • How does it handle Tapers or Insulin Scales?
Pilot Learnings • Very few of FRH patients with CHF/COPD were readmissions during pilot • Around 50% weren’t associated with Fairview Clinics • The clinic care coordinator needs to control the management of these patient populations • Communication with hand off information is essential • A minimum of 1 home care visit within 24-48 hours post hospitalization is necessary to ensure safe transition to home
FPA/UCare • Two primary interventions • Pharmacy Discharge Reconciliation • Follow up visit with Primary Care within five days • Excellent outcomes demonstrated • 30 day readmissions decreased by 42% • Relatively low cost to administer • Expanding to other facilities
UMMC Pediatrics • Intensive Discharge Reconciliation and Education • Post-discharge follow up calls • 75% capture rate for prescriptions • No readmission data demonstrated yet • Excellent customer satisfaction
Which Patients? • Everyone? • High-risk Diagnoses (and high risk for what…)? • CHF/COPD • Pneumonia • AMI • High-Risk Medication Therapies or Regimens? • Particular Payers? • Risk Stratification?
Hotspotting “The critical flaw in our health-care system…is that it was never designed for the kind of patients who incur the highest costs. Medicine’s primary mechanism of service is the doctor visit and the E.R. visit. (Americans make more than a billion such visits each year, according to the Centers for Disease Control.) For a thirty-year-old with a fever, a twenty-minute visit to the doctor’s office may be just the thing. For a pedestrian hit by a minivan, there’s nowhere better than an emergency room. But these institutions are vastly inadequate for people with complex problems: the forty-year-old with drug and alcohol addiction; the eighty-four-year-old with advanced Alzheimer’s disease and a pneumonia; the sixty-year-old with heart failure, obesity, gout, a bad memory for his eleven medications, and half a dozen specialists recommending different tests and procedures. It’s like arriving at a major construction project with nothing but a screwdriver and a crane.” New Yorker Article by Atul Gawande http://www.newyorker.com/reporting/2011/01/24/110124fa_fact_gawande
ETG/ERG Risk Scoring • Episode Treatment Groups • Groups various encounters based on disease “episodes” • Episode Risk Group • Assigns a “risk score” to each episode based the associated diagnosis • Average patient score is 1 • Higher scores are “sicker” patients, lower scores are “healthier” • Scores are used to predict future healthcare utilization
Readmission Risk vs. ERG Score (n = 100 patients)
Inpatient Hospitalization TCU/SNF/Home Care/Home Primary Care