Download
1 / 37
370 likes | 395 Views
Staphylococci are significant Gram-positive bacteria, including major pathogen Staphylococcus aureus. Learn about their habitats, diseases they cause, and antibiotic resistance patterns.

E N D
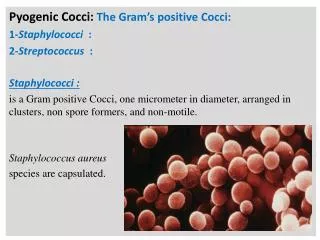
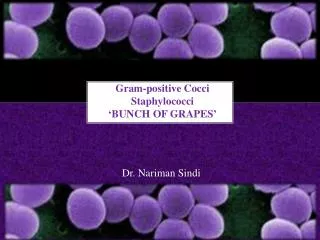
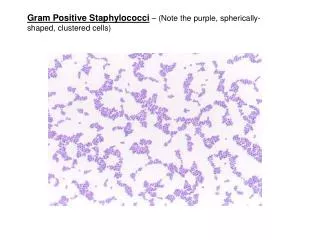
INTRODUCTION • Staphylococci are Gram-positive spherical bacteria arranged in microscopic clusters resembling grapes • Staphyloccocci – Greek word “stapyle” =bunch of grapes and “kokkos”= a berry. • This group includes a major human pathogen and skin commensals
Grouping for Clinical Purposes • Coagulase positive Staphylococci • Staphylococcus aureus- major pathogen • Coagulase negative Staphylococci • Staphylococcus epidermidis • Staphylococcus saprophyticus • Staphylococcus hemolyticus
Staphylococcus aureus • Major human pathogen • Habitat - S. aureus colonizes mainly the nasal passages, but it may be found regularly in most other anatomical sites, including skin, oral cavity and gastrointestinal tract • Source of organism - can be infected human host, carrier, fomite or environment
Culture: S.aureus forms a fairly large golden yellow colony on rich medium • Often hemolytic on blood agar • S.aureus- golden yellow colonies • S.albus- white colonies • S.citreus-lemon yellow colonies
Biochemical reactions: • Staphylococci are facultative anaerobes that grow by aerobic respiration or by fermentation that yields principally lactic acid • Catalase-positive
Nearly all strains of S. aureus produce the enzyme coagulase • S.aureus should always be considered a potential pathogen
Important phenotypic characteristics of S.aureus • Gram-positive, cluster-forming cocci • facultative anaerobe -fermentation of glucose produces mainly lactic acid • Catalase positive, Coagulase positive • Golden yellow colony on agar • Normal flora of humans found on nasal passages, skin and mucous membranes • Pathogen of humans: causes suppurative infections, food poisoning, toxic shock syndrome
Natural history of disease • Neonates, children, adults -intermittently colonised by S. aureus • Usual sites - skin, nasopharynx, perineum • Breach in mucosal barriers - can enter underlying tissue- Characteristic abscesses • Disease due to toxin production
DISEASES Due to direct effect of organism • Local lesions of skin • Deep abscesses • Systemic infections Toxin mediated • Food poisoning • Toxic shock syndrome • Scalded skin syndrome
Factors predisposing to S. aureus infections Host factors • Breach in skin • Chemotaxis defects • Opsonisation defects • Neutrophil functional defects • Diabetes mellitus • Presence of foreign bodies Pathogen Factors • Catalase (counteracts host defences) • Coagulase • Hyaluronidase • Lipases • B –lactasamase (antibiotic resistance)
SKIN LESIONS • Boils, Styes • Furuncles (infection of hair follicle) • Carbuncles (infection of several hair follicles) • Wound infections • Impetigo (skin lesion with blisters that break and become covered with crusting exudate)
DEEP ABSCESSSES • Can be single or multiple • Breast abscess can occur in 1-3% of nursing mothers in puerperium • Other sites - kidney, brain from septic foci in blood
Systemic Infections • Osteomyelitis, septic arthritis • Heart (infective endocarditis) • Brain(brain abscesses) • With predisposing factors • multiple abscesses, septicaemia (IV drug users) • Staphylococcal pneumonia (Post viral)
B. TOXIN MEDIATED DISEASES Staphylococcal food poisoning • Due to production of entero toxins- heat stable entero toxin acts on gut • Produces severe vomiting following a very short incubation period • Resolves on its own within about 24 hours
Toxic shock syndrome • High fever, diarrhoea, shock and erythematous skin rash which desquamate • Mediated via ‘toxic shock syndrome toxin’ • 10% mortality rate • Described in two groups of patients • Young women using tampones during menstruation • Described in young children and men
Scalded skin syndrome • Disease of young children • Mediated through minor Staphylococcal infection by ‘epidermolytic toxin’ producing strains • Mild erythema and blistering of skin followed by shedding of layers of epidermis
Antibiotic sensitivity pattern • Very imp. In Pt. Management • Antibiotic resistance mechanisms • Β-lactamase production - plasmid mediated • Has made S. aureus resistant to penicillin group of antibiotics - 90% of S. aureus • B lactamase stable penicillins (cloxacillin, oxacillin, methicillin) used
Alteration of penicillin binding proteins- (Chromosomal mediated) • Has made S. aureus resistant to β-lactamase stable penicillins (MRSA) • 10-20% S. aureus are resistant to all Penicillins and Cephalasporins • Vancomycin is the drug of choice
MRSA detected in the lab using methicillin • In Japan emergence of VIRSA(vancomycin intermediate resistant S. aureus) • No effective antibiotics for successful treatment
DIAGNOSIS • In all pus forming lesions • Gram stain and culture of pus • In all systemic infections • Blood culture • In infections of other tissues • Culture of relevant tissue or exudate
Staphylococcal Lab Identification & Diagnostic Tests • Microscopic • Lab isolation • Coagulase positive • S. aureus
Mannitol Salt Agar (MSA) Staphylococcus aureus
Differential Characteristics Catalase 2H2O2 O2 + 2H2O Streptococcivs. Staphylococci
Catalase POS Catalase NEG Staphylococcus
S. aureus Differential Characteristics Coagulase Fibrinogen Fibrin
Staphylococcus aureus Coagulase POS Coagulase NEG
Treatment • Drain infected area • Deep/metastatic infections • Semi-synthetic penicllins • Cephalosporins • Erythromycin, Clindamycin • Endocarditis • semi-synthetic penicillin + an aminoglycoside • MRSA: Vancomycin
Prevention • Carrier status prevents complete control • Proper hygiene, segregation of carrier from highly susceptible individuals • Good aseptic techniques when handling surgical instruments • Control of nosocomial infections
2. Staphylococcus epidermidis • Skin commensal • Has predilection for plastic material • Ass. With infection of IV lines, prosthetic heart valves, shunts • Causes urinary tract infection in cathetarised patients • Has variable ABS pattern • Treatment should be aided with ABST
3. Stapylococcus saprophyticus • Skin commensal • Imp. Cause of UTI in sexually active young women • Usually sensitive to wide range of antibiotics