Download
1 / 43
480 likes | 1.28k Views
Gram-positive Cocci Staphylococci ‘BUNCH OF GRAPES’. Dr. Nariman Sindi. Gram-positive Cocci. Coccus ‘ Spherical shape ’. Two medically important genera of gram-positive cocci: Staphylococcus and Streptococcus and are responsible for a wide variety of clinical diseases.

E N D
Gram-positive Cocci Staphylococci‘BUNCH OF GRAPES’ Dr. Nariman Sindi
Gram-positive Cocci • Coccus ‘ Spherical shape’. • Two medically important genera of gram-positive cocci: Staphylococcus and Streptococcusand are responsible for a wide variety of clinical diseases. • Staphylococci appear in grapelike clusters, whereas streptococci are in chains.
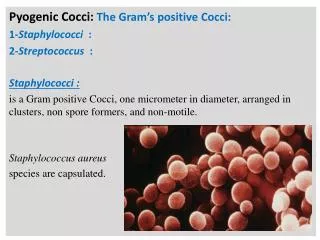
STAPHYLOCOCCUS • The most important species associated with human diseases: • Staphylococcus aureus (S. aureus). • Staphylococcus epidermidis (S. epidermidis). • Staphylococcus saprophyticus(S. saprophyticus).
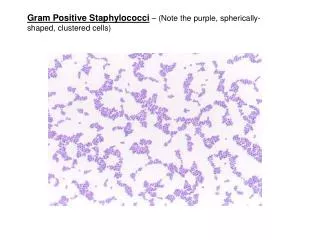
PROPERTIES • Characteristics: • Spherical gram-positive cocci arranged in grapelike clusters. • Catalase-Test: positive (degrades H2O2 into O2 and H2O). • Coagulase-Test: positive (coagulase activates pro-thrombin to form thrombin, causing blood to clot). • β-hemolytic (completely hemolyze RBCs on an agar plate). • Facultative anaerobic. • Non-spore forming. Gram stain of S. aureus cells which typically occur in clusters
PROPERTIES • Habitat and Transmission: • Main habitat: • Exist as a normal flora on skin and mucosal surfaces of human. • S. aureus is also found in the vagina of approximately 5% of women. • All over hospitals. • Transmission: • Staphylococcus aureus is always spread by physical contact, not through the air. • Staphylococcus aureus can spreaddirectlyfrom the pus of an infection like boils or abscesses through skin-to-skin contact. • Through indirect contact with contaminated objects such as sheets, towels, sport equipment. • Presence of foreign body (suture, catheter). • Unnecessary antibiotic use for years. • Staphylococcus aureus can survive on dry surfaces for up to several months.
Virulence factors • S. aureus has numerous powerful weapons stick out of the microcapsule: • Protein A:This protein has sites that bind immunoglobulin IgG, preventing opsonization and phagocytosis. • Coagulase: Allows fibrin formation around organism, protecting it from phagocytosis. • Catalase.Conversion of hydrogen peroxide to water and oxygen. • Hemolysins:β-hemolysis (complete lysis of red blood cells) on an agar plate which appears as a yellow golden pigment on sheep blood agar. Hemolysins destroy RBCs, macrophages, and platelets.
Virulence factors • Leukocidins:Destroy leukocytes (WBCs). • Penicillinase (β-lactamase):This enzyme produced by S. aureus that provide resistance to beta-lactam antibiotics like penicillins.It disrupt the beta-lactam portion of the penicillin molecule, thereby inactivating the antibiotic by breaking the antibiotics' structure. • Hyaluronidase:Breaks down connective tissue facilitating S. aureus spread in tissue. • lipases:Degrades fats and oil on the surface of our body. This degradation facilitates S. aureus’ colonization of glands. • Protease:Destroys tissue proteins.
Clinical diseases • Staphylococcus aureus causes a wide range of human diseases which can be separated into two groups: • Diseases Caused By Exotoxin Release. • Disease Resulting From Direct Organ Invasion. • Diseases Caused By Exotoxin Release: • Enterotoxin (Gastroenteritis, food poisoning): • Staphylococci can grow in food produce an exotoxin (e.g., ham, pastries, potato salad, and ice cream). • The victim will then eat the food containing the pre-formed toxin. • Rapid onset of disease within 4 hours. • Food poisoning characterized by vomiting, watery diarrhea, abdominal pain, and occasionally fever. Lasts 12 to 24 hours.
Clinical diseases • Toxic Shock Syndrome Toxin-1 (TSST-1): • TSST-1 causes toxic shock, especially in tampon-using menstruating women. • TSST is produced locally by S. aureus in the vagina. The toxin release into the blood stream, causing a toxemia causes high fever, nausea and vomiting, watery diarrhea, and rash. • This diseases may involve three or more organs: liver, kidney. Muscle, blood, gastrointestinal, or central nervous system (CNS). • ‘Staphylococcal Scalded Skin Syndrome (SSSS) or ‘Ritter’s disease’. • A Staphylococcus aureus strain, which produces exfoliative toxin A and B. • It is characterized by fever, rash, hair and nails can be lost. Recovery usually occurs within 7-10 days. • Usually affects neonates and young children.
Clinical diseases Scalded skin syndrome (SSS) TSST-1
Clinical diseases B. Disease Resulting From Direct Organ Invasion: • Local infection: • Skin infection are very common. • Impetigo: • usually occurs on the face, especially around the mouth. • Small vesicles lead to pustules. • Cellulitis: • This is a deeper infection of the cells. • The tissue becomes hot, red, shiny and swollen.
Clinical diseases • Local Abscesses, Furuncles, and Carbuncles: • Abscesses is a collection of pus. Infection of hair follicle produces pus with a red rim. This infection can penetrate deep into the subcutaneous tissue to become a furuncle. These may produce painful lesions communicating under the skin called carbuncles. • Wound infections: • Any skin wound can be infected with S. aureus after surgical procedure. • Their clinical signs are: increasing local pain, redness, swelling. • It must be reopened the wound and remove the foreign matter. • If the wound does not heal, antibiotic therapy should be used against S. aureus.
Abscesses Wound infection Furuncle Carbuncles
Clinical diseases • Systemic diseases: • Pneumonia: • S. aureus pneumonia usually follows a viral influenza (flu) upper respiratory illness, with onset of fever, chills, rapid destruction of lung, resulting in cavitaions (holes in the lung), and pus. • In many hospitals, S. aureus is the most common cause of nosocomial pneumonia. • Meningitis, Cerebritis, Brain Abscess: • These patients can present with high fever, stiff neck, headache, coma, and neurologic signs.
Clinical diseases Staphylococcus aureus pneumonia
Clinical diseases • Osteomyelitis: • This is a bone infection that usually occurs in boys <12 years of age. • The infection spreads to the bone, presenting locally with warm, swollen tissue over the bone, fever, and shakes. Osteomyelitis
Clinical diseases • Arthritis: • Invasion of the synovial membrane by Staphylococcus aureus. • Patients complain of painful red swollen joints with decreased range of motion. • S. aureus is the most common pathogen causing this disease in children and adults over the age of 50. • Without prompt treatment, many patients will permanently lose the function of the joints. • Antimicrobial therapy is required.
Clinical diseases • Endocarditis: • This is a destructive infection of the heart valves. • A sudden onset of high fever, chills, and myalgia. • Intravenous drug (IV) users develop endocarditis. • Blood and catheter infection: • Staphylococcus aureus can migrate from the skin and colonize central venous catheters resulting in bacteremia, sepsis, and endocarditis.
MRSA is Methicillin-Resistant Staphylococcus aureus. • More than 90% of S. aureus contain plasmid that encode β-lactamase (penicillinase) which provide resistance to antibiotics such as penicillinase-resistant penicillins (methicillin, nafcillin, oxacillin, etc.). • MRSA is a dangerous type of S. aureus causes skin and other infections. • MRSA tend to develop in the hospital, where broad spectrum antibiotics are used. • MRSA is spread by the hand contact with another infected patient, sharing personal items (towels, razors, etc.), touching surface or items contaminated with MRSA. MRSA FACT SHEET
pathogenesis • Different toxins and enzymes are produced by S. aureus. There are three clinically important exotoxins are exfoliation, enterotoxins, toxic shock syndrome toxin-1 (TSST-1). • Exfoliationseparate the epidermis at the granular cell layer causes ‘scalded skin syndrome’ in young children. • Enterotoxins cytokines released from the lymphoid cells stimulate the nervous system to activate the vomiting center in the brain. • TSST-1 tampon-using menstruating women left for long time stimulate S. aureus to release the exotoxin TSST-1 penetrate the vaginal mucosa stimulate the release of large amount of IL-1, IL-2, and tumor necrosis factor (TNF) high fever, diarrhea, vomiting, rash.
Laboratory diagnosis • Serious staphylococcal infections such as infection of the bloodstream, pneumonia, and endocarditis require culturing of samples of blood or infected fluids. • Infected wound (either a small biopsy of skin or pus taken with a swab) or of the blood must be obtained to grow the bacteria in the microbiology laboratory. Once the Staph is growing, the organism is tested to determine which antibiotics will be effective for treating the infection.
Laboratory diagnosis • Gram Stain:S. aureus lie in grape-like clusters as seen on gram stain. Staphylococcus aureus is a typical Gram-positive bacterium forming irregular clusters of cocci.
Laboratory diagnosis 2) Culture: • β-hemolytic. • Produces a golden yellow pigment on sheep blood agar. Staphylococcus aureus cultivated on Columbia agar with 5% defibrinated sheep blood. Cultivation 24 hours in an aerobic atmosphere, 37°C. Colonies are surroundend by a wide zone of beta-hemolysis. Yellow pigmented colonies of Staphylococcus aureus, Columbia agar with 5% defibrinated sheep blood. Cultivation 24 hours, aerobic atmosphere, 37°C. Colonies are surroundend by a wide zone of beta-hemolysis.
Laboratory diagnosis 3) Metabolic: • Catalase Test: positive. • Coagulase Test: positive (Slide coagulase test, tube coagulase test). Tube coagulase-positive, clot plasma into gel and do not flow when inverted Catalase test-positive (blowing oxygen bubbles) Slide coagulase-positive
treatment • Approximately 90% of S. aureus strains are resistant to penicillin G because they secret penicillinase (β-lactamase). Less than 10% of the strains are susceptible to this antibiotic. • Penicillinase-resistant penicillins (IV): • These strains of β-lactamase-resistant penicillin can be treated with nafcillin or methicillin. Unfortunately, S. aureus strains quickly developed resistance to these antibiotics. These resistant strains are often abbreviated NRSA or MRSA respectively. • The drug of choice for these staphylococci is vancomycin. However, intermediate resistance (VIRS) and complete resistance (VRSA) to vancomycin have been isolated from patients.
treatment • Synercid: • At this time, a combination of two antibiotics, Quinupristin/dalfopristin (brand name ‘Synercid’) • It is used to treat certain serious bacterial infections that have not responded to treatment with other antibiotics (resistant infections). • It is inhibit the growth of bacteria. • This medication is given by injection, usually 2 to 3 times daily
prevention • Vaccine is NOT currently available against Staphylococcus aureus. • Practicegood hygiene, with careful hand washing. • cleancuts, scrapes, and wounds. • Usedisposable gloves, especially in hospitals and nursing homes, to avoid skin-to-skin contact. • Avoid skin contact with an infected person. • Useethanol as a topical sanitizer against MRSA. • Useproper food handling and preparation to prevent food poisoning.
properties • Characteristics: • Gram positive cocci in clusters. • Catalase test-positive. • Coagulase test-negative. • Habitat and Transmission: • Habitat: normal flora of the human skin and mucosal membranes. • Transmission: via hands.
virulence factors • Polysaccharide Capsule:adhere to a variety of prosthetic devices such as prosthetic joints, prosthetic heart valves, and peritoneal dialysis catheters. • Highly resistant to antibiotics. • Clinical diseases • S. epidermidis enters the blood stream causing bacteremia. • Infections of intravenous catheters sites and prosthetics materials such as prosthetic heart valves (endocarditis), prosthetic joints (arthritis or osteomyelitis), sepsis in neonates, and large wounds. • It is the major cause of hospital acquired infections. Itis very likely to contaminate patient-care equipment and environmental surfaces. • Unlike, S. aureus, no toxins have been identified.
Laboratory diagnosis • Gram stain: • Gram positive cocci in clusters. • Culture: • Whitish, non-hemolytic colonies on blood agar Golden S.aureusand white S.epidermidis colony
Laboratory diagnosis • Metabolic: • Catalase test-positive. • Coagulase test-negative. • Antibiotic test: • Sensitive to novobiocin antibiotic Catalase-test positive Novobiocin-sensitive
treatment • The drug of choice is vancomycin, to which either rifampin or an aminoglycoside can be added. • S. epidermidis is highly resistant to antibiotics, because the production of beta-lactamase. PREVENTION • There is no drug or vaccine available.
properties • Characteristics: • Gram positive cocci in clusters. • Catalase test-positive. • Coagulase test-negative. CLINICAL DISEASES • Urinary tract infection in women.
Laboratory diagnosis • Gram stain: • Gram positive cocci in clusters. • Culture: • Gamma-hemolytic. • Metabolic: • Catalase test-positive. • Coagulase test-negative. • Antibiotic test: • Resistant to novobiocin antibiotic Novobiocin-resistant
treatment • Norfloxacin used to treat urinary tract infection.
Gram Positive Cocci GPC Catalase-test H2O2 into O2 and H2O Staphylococci
Coagulase-test S. aureus S. epidermidis or S. saprophyticus Novobiocin Methicillin R S R S. epidermidis S. saprophyticus MRSA