Download
1 / 96
1k likes | 1.22k Views
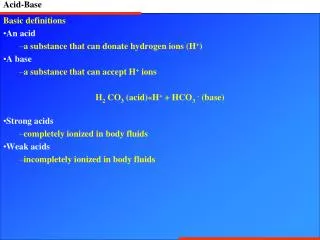
ACID BASE PATHOPHYSIOLOGY AND DISEASE STATES. Disorder pH pCO 2 [HCO 3 - ]. The Four Cardinal Acid Base Disorders. M acidosis . . M alkalosis. . R acidosis . . R alkalosis. . Alb -. ~ 10-12 mM/L. HCO 3 -. Na +. Cl -.

E N D
Disorder pH pCO2 [HCO3-] The Four Cardinal Acid Base Disorders M acidosis M alkalosis R acidosis R alkalosis
Alb- ~ 10-12 mM/L HCO3- Na+ Cl- Metabolic Acidosis: The “Anion Gap” [Na+] - ([Cl-] + [HCO3-])
Na+ + Cl- + H+ + HCO3- Na+ + Cl- +H2CO3 Na+ + Cl- +CO2 + H2O What happens after HCl addition: Na+ + Cl-
Alb- Alb- HCO3- HCO3- Na+ Na+ Cl- Cl- Nl Anion gap M acidosis Metabolic Acidosis: The “Anion Gap” [Na+] - ([Cl-] + [HCO3-])
Na+ + A- + Cl- + H+ + HCO3- Na+ + A- +Cl- +H2CO3 Na+ + A- +Cl- +CO2 + H2O What happens after AH addition where “A” is a retained anion: Na+ + A- +Cl-
Alb- Alb- Alb- HCO3- HCO3- HCO3- A- Na+ Na+ Na+ Cl- Cl- Cl- High Anion gap M acidosis Metabolic Acidosis: The “Anion Gap” [Na+] - ([Cl-] + [HCO3-]) Nl Anion gap M acidosis
Na+ Cl- BUN K+HCO3- creatinine Glucose 140 105 30 4.5 25 1.5 90 Clinician short-hand you should know:
And now, it’s time for: “Calculate That Gap” 140 105 30 Glucose 90 4.5 25 1.5 140 -(105 + 25) = 10 = normal 141 105 27 Glucose 100 4.2 6 1.2 141 - (105 + 6) = 30 = high 139 113 33 Glucose 126 3.7 16 1.4 139 - (113 + 16) = 10 = normal
Differential Dx of high-anion • gap acidosis: "SLUMPED": • Salicylates • Lactic acidosis • Uremia • Methanol intoxication • Paint sniffing (toluene) • Ethylene glycol intoxication • DKA or alcoholic ketoacidosis
Salicylates - ± Hx aspirin ingestion, nausea, tinnitus, unexplained hyperventilation, noncardiogenic pulmonary edema, elevated prothrombin time Usually: mixed respiratory alkalosis & metabolic acidosis (rare: metab pure acidosis) Toxic at < 5 mEq/l, so no anionic contrib to AG No increase in osmolal gap ([ASA] < 5 mM)
Treatment for salicylate intoxication: Un-ionized form (protonated) enters the brain and is excreted poorly So….alkalinize (HCO3 infusion) to maximize renal excretion (dialysis)
Lactic acidosis - Type A = increased O2 demand or decreased O2 delivery Type B = Malignancies (lymphoma) Phenformin, metformin hepatic failure acute respiratory alkalosis (salicylates) HAART congenital (glycogen storage disease type I) etc
Uremia is indicated by BUN, creatinine (chronicity by kidney size and Hct). Methanol - presents with ± abdominal pain, vomiting, headache; CT: BL putamen infarcts visual disturbance (optic neuritis)
Putamen infarcts Methanol intoxication: neurological effects Normal retina (left); optic neuritis (right)
Anion gap may be > 50 Osmolal gap > 10 mOsm
Paint sniffing (“huffing”) (toluene) may present as either anion gap acidosis or normal gap acidosis Anion = hippurate No increase in osmolal gap
Ethylene glycol - presents with ± CNS disturbances, cardiovascular collapse, respiratory failure, renal failure Oxalate crystals (octahedral or dumbell) in urine are diagnostic Anion gap may be > 50 Osmolal gap > 10 mOsm
“The rotund rodents chew through brake lines and radiator hoses in search of a fix of ethylene glycol…” “Marmots have an amazing ability to handle toxic substances. To tranquilize them, they need the same dose as a bear, and a bear will be down for 40 minutes while a marmot will be back up in 5. If you have to redrug them, it’s really hard to make them unconscious again.” National Wildlife Feb/Mar, 2002
Oxalate crystals “back of the envelope”
Treatment for methanol & ethylene glycol intoxication: 1. Ethanol infusion to compete with alcohol dehydrogenase (dialysis) OR 2. “Antizol” (fomepizole) (inhibits ADH) load, then 10 mg/kg q12 x 4
Diabetic ketoacidosis - Key clinical features are: type I DM (i.e. no insulin) a trigger: e.g. sepsis, fracture, stroke hyperglycemia ECF vol depletion & renal insufficiency acetoacetic- and hydroxybutyric- acids
Alcoholic ketoacidosis - key clinical features are recent stopping ingestion of ethanol, hypoglycemia, and contracted ECF (usually due to vomiting)
THE SERUM OSMOLALITY CAN HELP WITH THE DIAGNOSIS IN HIGH ANION GAP ACIDOSES Step 1: Calculate Osm = 2[Na+] + glucose/18 + BUN/2.8 Step 2: Measure Osm (freezing point depression) 3. Osmolal gap (measured - calc) should be ≤ 10 Osm gap due to small, osmotically-active molecules: mannitol (no acidosis) ethanol (acidosis = AKA) isopropanol (a "drunk" with ketones, but no acidosis) methanol (acidosis) ethylene glycol (acidosis)
Does metabolic acidosis cause hyperkalemia via H+/K+ exchange?
Na+ + Lact- +Cl- +CO2 + H2O Lact- HCO3- Na+ + Lact- + Cl- + H+ + HCO3- Na+ + Lact- +Cl- +H2CO3 Acute lactic acidosis from seizures (“closed” system”; lactate reabsorbed) Na+ + Cl- + HCO3- Na+ + Lact- +Cl- (low HCO3-,high gap) Na+ + Cl- + HCO3- (normal HCO3-,normal gap)
[HCO3-] pH A. Gap [K+] Seizure Acute lactic acidosis from seizures (“closed” system”; lactate reabsorbed) Time (minutes)
H+ H+ A- Cl- K+ K+ Principles of K+/H+ Exchange: 1. Occurs if anion is impermeable 2. Limited if anion is permeable (“organic”)
Causes of a “normal anion gap” (A.K.A. “hyperchloremic”) metabolic acidosis 1. GI bicarbonate loss: diarrhea villous adenoma pancreatic, biliary, small bowel fistulae uretero-sigmoidostomy obstructed uretero-ileostomy
HCO3- HCO3- HCO3- Cl- Cl- HCO3- K+ Diarrhea Causes Loss of HCO3- And a Normal Anion Gap Acidosis And Hypokalemia Pancreas Pancreas Ileum Ileum Colon Colon Cl- Normal Diarrhea
Na+ Na+ K+ K+ HCO3- Cl- K+ Flooding the colon or CCD with HCO3- instead of Cl- drives K+ secretion
HCO3- Cl- Pancreatic fistula or transplant: loss of HCO3- Pancreas Ileum Skin or urinary bladder
Cl- Cl- Obstructed Uretero-ileostomy Causes a Normal Anion Gap Acidosis Skin HCO3- Ureter Obstructed ileal loop Ileal loop Ileostomy bag
How to differentiate GI HCO3- loss from renal HCO3- loss? Use the urinary anion gap The underlying assumption is that NH4+ is excreted and maintains electroneutrality: ([Na+] + [K+] + [NH4+]) - [Cl-] = 0 Since NH4+ is unmeasured, a negative urine anion gap indicates NH4+Cl excretion (i.e. normal renal tubule acidification)
A positive urine anion gap ~ no NH4+Cl excretion (i.e. low renal tubule acidification) Normal acidotic: closed circles Diarrhea: closed triangles Type 1 or IV RTA: open circles Battle et al, NEJM 1988
Causes of a “normal anion gap” (A.K.A. “hyperchloremic”) metabolic acidosis 2. Ingestions & infusions ammonium chloride hyperalimentation (arginine/lysine-rich) 3. Renal bicarbonate (or equivalent) loss proximal RTA distal RTA type IV RTA early renal failure acetazolamide hydrated DKA
Na+ (1) Na+ HCO3- H+ H+ (3) HCO3- + CO2 H2O Na+ Defective Na+ - dependent resorption = Fanconi’s Syndrome Proximal RTA (“Type II”) HCO3- glucose amino acids urate phosphate
Autosomal recessive SLC4A4 NBC1 Prox RTA corneal Ca++ pancreatitis Autosomal recessive CA2 Carbonic Anhydrase II Proximal Or distal Or “hybrid” RTA; osteopetrosis; cerebral Ca++ Genetically-Defined Proximal RTAs Inheritance Gene Gene product Clinical features
filtered UHCO3V UHCO3V New HCO3 Tm HCO3-Tm Type II Renal Tubular Acidosis (“Proximal RTA”) HCO3- in moles/time GFR x [HCO3-]plasma = “filtered load of HCO3-”
HCO3- Type II Renal Tubular Acidosis (“RTA”)
NH4+ NH3 Not titratable; need to measure + H2PO4- HPO4-- + + HCO3- Titratable acid H2CO3 Present in Prox RTA Net acid excretion = urinary NH4+ + urinary “titratable acid” (H2PO4-) - urinary HCO3- H+
Flooding of CCD with HCO3- exceeds its resorptive capacity; HCO3- becomes “a poorly resorbed anion” Na+ Na+ HCO3- K+ K+ Principal cell ATP Cl- H+ HCO3- HCO3- ADP + Pi Cl- Cl- a IC cell ATP H+ ADP + Pi pHmin = 5 Cl- b IC cell
HCO3- HCO3- HCO3- K+ HCO3- K+ How Diarrhea and Proximal RTA Are Alike Glomerulus Pancreas Ileum Prox tubule CCD Colon
Fractional excretion of HCO3- in proximal RTA
Features of Proximal Renal Tubular Acidosis (“Type II”) Diminished proximal resorption of HCO3- Plasma [HCO3-] 10-15 mEq/L Urine pH depends on plasma [HCO3-] & GFR relative to proximal HCO3- Tm Fractional HCO3- excretion high (15-20%) at nl plasma [HCO3-] Plasma [K+] reduced, worsens with HCO3- therapy Dose of daily HCO3- required: 10-15 mEq/kg/d Non-renal: rickets or osteomalacia
Causes of a “normal anion gap” (A.K.A. “hyperchloremic”) metabolic acidosis 3. Renal bicarbonate (or equivalent) loss proximal RTA distal RTA type IV RTA early renal failure acetazolamide hydrated DKA
Na+ Na+ K+ K+ Aldosterone Auto-immune ATP Cl- H+ HCO3- HCO3- ADP + Pi Cl- amphotericin Cl- ATP H+ ADP + Pi Cl- Distal RTA Principal cell a IC cell b IC cell
Na+ Na+ K+ K+ Aldosterone ATP Cl- H+ HCO3- HCO3- ADP + Pi Cl- Cl- ATP H+ ADP + Pi Cl- Hypo- kalemia in distal RTA: H + no longer shunts Na + current so K+ must do so Principal cell a IC cell b IC cell