Download
1 / 51
510 likes | 523 Views
Explore the anatomy of sinuses, functions, conditions like sinusitis, and imaging techniques for diagnosing sinus issues. Discover how sinuses impact our health and learn about essential sinus projections.

E N D
What is a sinus? • Cavity within a bone • Canal or passageway leading to an absess • dilated channel for venous blood • any cavity having relatively narrow opening
57 different kinds sinuses in human body! • Heart • Ankle • Brain • Coccyx • Spleen • Kidney • Uterus • Anus • Skull- around the nasal cavity known as….
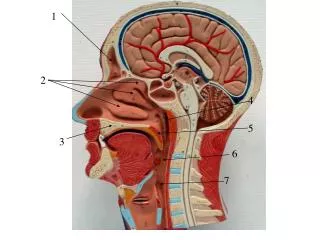
Paranasal Sinuses Each sinus is name after the bone it resides in!
Development • Start as small sacs around nasal meatus & recesses • Grow – invading bone- forming air sinuses and cells • Maxillary seen at birth
By age 6 or 7 frontals & sphenoids distinguish themselves • Ethmoids around puberty • All full developed age 17- 18 • All sinuses communicate nasal cavity and each other
Functionsof Paranasal Sinuses? • Not definitely known!-but speculated: • decrease weight of skull • resonating chamber for voice • help warm and moisten air • act as airbags in trauma • possibly control immune system
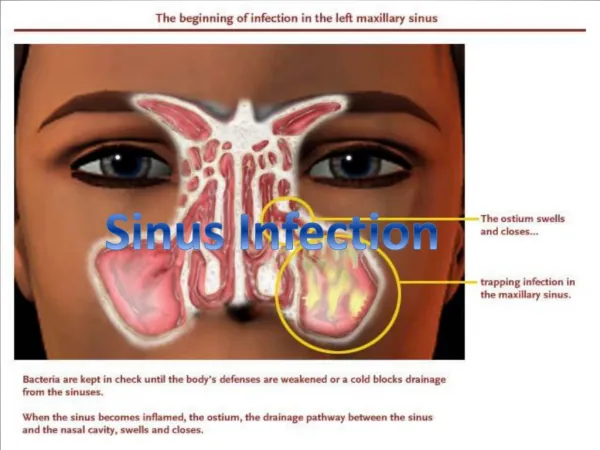
Paranasal sinuses are joined to nasal cavityvia small orifices calledOstia (harbour city of ancient Rome) Ostiaeasily blocked by allergic inflammation or swelling of nasal lining drainage of mucous is disrupted Sinusitismay result!
What is Sinusitis? • Inflammation of sinuses- caused by bacterial infection of membrane lining- can fill with pus! • Usually from common cold (after first attack, recurrence more likely) • Can spread from upper tooth infection • Jumping in infected water without holding nose
Symptoms of Sinusitis • Loss of smell • Fever • Fullness or tension • Pain • 37 million Americans suffer every year • Decongestion opens up ostia to restore drainage
Sinusitis Video (Click on icon)
Conditions aggravating Sinusitis • Scuba diving • Chlorinated swimming pools • Drinking alcohol • Airplane rides (vacuum)
What is Ex-u-date? (Something that exudes!) • Heavy, semi-gelationous material that likes to cling to walls of sinuses (Mucous) • Allow several minutes for material to layer out if going from erect projection to cross-table projection • Clean Image Receptor before and after!!
There are 4 sets of Paranasal Sinuses Frontal Maxillary Ethmoid Sphenoid
Frontal Sinuses 2nd Largest Usually paired-sometimes one, three or none! Great variation in size and shape-almost never symmetrical (califlower)
Maxillary Sinuses Largest (think Maximum!) Two, symmetrical but vary in size and shape from person to person Can be seen at birth Apices at bottom of sinus!
Ethmoid Sinuses Paired Divided into 3 groups- anterior- 2-8 cells middle- 2-8 cells posterior 2-6 cells 6-22 possible each side
Sphenoid Sinuses Paired (sometimes one) Great variation in size and shape Asymetric Directly below Sella turcica
Horizontal Beam Beam angles up 45 degrees
If patient cannot sit or stand upright, what is an alternative method for getting equally useful views? CrossTable Lateral or DorsalDecubitus
To see an anterior posterior projection-- A Lateral Decubitus!--As long as beam is horizontal, a fluid level can be demonstrated!
All sinuses views are performed- With a 40 “ SID Collimated to area of sinuses Erect (or crosstable) 8X10 cassette
4 Basics Projections of Sinus Series • PA Axial (Caldwell) • Parietoacanthial (Waters) • Lateral • SMV (basilar)
PA axial(Caldwell method) Incorrect! Beam should not be angled- must be horizontal! X
For proper PA axial of sinuses, eithertilt IR 15 degrees forward Or keep IR vertical, butextend pt.’s head back 15 degrees
PA axial (Caldwell) beam exits at nasion interpupillary line horizontal midsagital plane perpendicular to IR 8X10 cassette Collimated to sinuses Best projection for Frontal sinuses!
How to Judge if you have a good Caldwell projection? No rotation (equal distance between lateral border of skull and lateral border of orbit) Petrous ridges in lower 1/3 or orbit Close beam colimation
Parietoacanthial projection (Waters) Horizontal beam exits at acanthion chin touches IR, nose extends back 1/2” from IR Angle of orbito-meatal line is 37 degrees (mento-meatal line is perpendicular to IR) Best projection for Maxillary sinuses!
Proper Waters Position OML is 37 degrees to IR (cassette) Not OML 37 deg. to CR!
ImproperParietoacanthial Position Nose is touching-thus OML is not 37 degrees to IR This is actually a “Modified” Waters for imaging orbits, nasal bones
AnUnder-extendedWaters projection Petrous ridges do not sit directly below apices of Maxillary sinuses! Head needs to be extended back further Does patient have sinusitis?
Lateral Projection Shows all 4 sets of sinuses at once!
LateralSinus projection Shows all 4 sinus groups, - mainly for sphenoid Similar to lateral skull, but collimate to anterior half of skull CR ½” – 1” posterior to outer canthus furthest from film CR parallel to floor
Evaluation Criteria - Lateral Sinus No rotation of sella turcica Superimposed orbital roofs Close beam restriction
SMV (basal) projection Demonstrates Ethmoid & Sphenoid sinuses best!
SMV- Sinuses Similar to skull, but collimated to anterior 2/3 of skull CR horizontal, perpendicular to IOML CR enters 3/4 anterior to level of EAM
Alternate SMV Position? Often times, better to omit SMV, depending on patient’s condition & age Beam not horizontal!
Evaluation Criteria -SMV Sinuses Equal distance from lateral border of skull to mandibular condyles on both sides Mental protuberance superimposes Frontal bone Condyles anterior to petrous pyramids
Is this an acceptable Waters projection? • No! • Apices of Max. sinus must be immediately above petrous pyramids • The head is underextended!
How about this Waters? • No! • Head overextended! • Frontal and maxillary sinuses are foreshortened • Apices too high above petrous ridges
Technical Factors very important with sinuses! • More critical & misleading than any other part of body • Under penetration-miss pathology or simulate false conditions • Over penetration- burn out pathology • Need to see both bony structure and soft tissue
Overpenetrated Waters Where is the frontal sinus? A bit overextended as well Remove dentures!
Underpenetrated Is there fluid in apices or not?
Should you shield? • Federal government has reported placing a lead shield over a pt.’s pelvis does NOT significantly reduce gonadal exposure during skull imaging • Do it anyway!