Download
1 / 18
180 likes | 337 Views
Precautionary Savings to Manage Common Health Risks among the Poor. Jessica Pickett University of Pennsylvania. Research Problem. Poor households struggle with unpredictable out-of-pocket health expenses Recent trend towards government, NGO microinsurance Primarily hospitalization

E N D
Precautionary Savings to Manage Common Health Risks among the Poor Jessica Pickett University of Pennsylvania Insurance in combination with other financial services
Research Problem • Poor households struggle with unpredictable out-of-pocket health expenses • Recent trend towards government, NGO microinsurance • Primarily hospitalization • Pharmaceutical & outpatient expenses rarely covered • Even minor illness can reduce consumption in inefficient capital markets • Productivity losses from under-treatment • Future losses from high-interest loans or asset sales • Precautionary savings as an alternative • Constrained by biased beliefs, inattention & inconsistent preferences Insurance in Combination with Other Financial Services
Options for Risk Management Insurance in Combination with Other Financial Services
Savings & Health • Financial impact of illness is lower in households with access to rural deposit accounts in Indonesia (Gertler, Levine & Moretti, 2009) • Market women in Kenya with access to individual savings accounts spend less working capital on medical costs & more likely to receive treatment for malaria episodes (Dupas & Robinson, 2010) • But recent research on health-specific savings technologies with Kenyan ROSCAs (Dupas & Robinson, 2011) and the impact of saving reminders more generally (Karlan, McConnell, Mullainathan, & Zinman, 2011)suggests households systematically underestimate future treatment costs • Financial access is not enough to ensure savings – must also address behavioral constraints • Supported by observed demand for health savings & loan products among Indian SHGs and MFI clients in Burkina Faso (Reinsch & Ramirez, 2011) Insurance in Combination with Other Financial Services
Research Questions • Does outpatient spending affect household consumption? • Is there demand for insurance and/or precautionary savings for health? • Why don’t the poor currently save enough for that purpose? Hypothesis:Insurance should be supplemented with better savings vehicles to overcome biased beliefs, inattention, inconsistent preference & other behavioral constraints to manage common illness Insurance in Combination with Other Financial Services
Theoretical Context • Permanent income hypothesis predicts households should always opt for remedial treatment for health shocks & thus always prefer full insurance, if actuarially fair • Predicts positive savings rate when insurance markets are not feasible or loading exceeds household’s willingness to pay • Assuming reasonable levels of risk aversion & interest rates • But precautionary savings for health still entails significant uncertainty • Exact timing even of frequent illnesses is unpredictable • Savings goals require accurate information on probability & costs of illness, as well as treatment efficacy • Households must diligently deposit savings & protect those funds from expropriation • Limited attention, narrow framing & commitment • Model of healthcare utilization under these forecasting constraints predicts negative savings rate & decreased future consumption due to asset sales, loans or decreased productivity Insurance in Combination with Other Financial Services
Expected Utility Model • Wage rate Yi, productive assets At, debt Dt & non-medical consumption Ct • Insurance at given loadingα • Disability-adjusted labor Ht determined by exogenous probability of illness & depreciation • Superscripts denote realized incidence of illness: 1 indicates a state of the world if sick & 0 if healthy • Remedial treatment at price pm Current period earnings Loan payments Medical expenses Insurance premium Insurance in Combination with Other Financial Services
Behavioral Model (Savings) • Forecast illness with probability) due to: • Inattentionor poor cognition • Imperfect information, innumeracy or biased beliefs • Disutility from considering negative prospects Current utility of full health Current period utility from illness Expected forecast of future utility Current period earnings Medical expenses Loan payments Insurance in Combination with Other Financial Services
Community-Based Savings Groups • Model suggests demand for savings products that would allow households to save to smooth consumption against health shocks • Ongoing research proposes the use of reminders, conditions & restrictions targeting individual accounts • Alternatively, existing community-based savings groups (CBSGs, aka VSLAs) “nudge” members to save more than simply increasing access to financial services • CBSG meeting structure and corresponding social dynamics simultaneously serve to maximize trust while mitigating many crucial behavioral constraints: • Mandated savings implicitly represents target savings goal & explicitly reminds members to save (compounded by peer effects) • Salience of medical costs & other financial risks is amplified by observing other members apply for loans or receive social fund grants • Reduces “negative” expropriation of funds by others by introducing formal loan structure where loans are likely to be repaid & member has access to liquid capital during interim • Loan requests subject to approval by the group, serving as a semi-liquid commitment device protecting against temptation goods or time-inconsistent preferences • Better way to manage outpatient expenses than ROSCAs or MFIs, where existing health savings pilots observed demand for health-specific accounts • But still subject to information problems Insurance in Combination with Other Financial Services
Case Study: Tajikistan Insurance in Combination with Other Financial Services
Case Study: Tajikistan • Poor, land-locked country in post-Soviet Central Asia; rural & mountainous, with a population of 7 million • Few natural resources; economy is heavily dependent on agriculture & remittances • Per capita income $1,860 (PPP); 47% poverty rate; GDP growth of 3.4% per year • High education levels & 100% literacy rate in Tajik (Persian) or Russian • Communicable disease ~ 72% of the overall disease burden, especially TB (MDR) • Crumbling Soviet health system: ostensibly free network of government-run hospitals (61 beds per 10,000) & salaried doctors (20 per 10,000) • Unsustainable excess institutional capacity • Vast majority of health costs paid out-of-pocket, mostly for pharmaceuticals, transportation & informal payments to government providers • 64% of households rate it “difficult” or “impossible” to find money for needed treatment • Aggravated by inefficient capital markets (17% interest rate spread) • Rural households lack access commercial banks, especially for relatively small transactions • MFIs increased access to credit but prohibited from accepting deposits or insurance products • Recent, widespread expansion of CBSGs has potential to mitigate these challenges Insurance in Combination with Other Financial Services
Case Study: Tajikistan Insurance in Combination with Other Financial Services
Data • Existing: Tajik Living Standards Survey (TLSS) contains data on household health expenditures, consumption & financial access • Nationally representative sample of 4,860 households in 2007 (stratified by region & population density) • WB Living Standards & Measurement Survey research program • Subset of panel data from 1503 households (10,069 individuals) in 2009 • 3rdwave of data collection began in November 2011 • Proposed:Detailed health & expenditure logs • Sub-sample of TLSS participants via SMS or phone interviews • “Large T” analysis can dramatically increase power with more frequent observations of a smaller overall sample for health outcomes, household expenditures & other noisy outcomes with low autocorrelation (McKenzie, 2011) • Also important given recall bias for frequent health spending (Das, Hammer & Sanchez, 2012) • CBSG expansion as a natural experiment Insurance in Combination with Other Financial Services
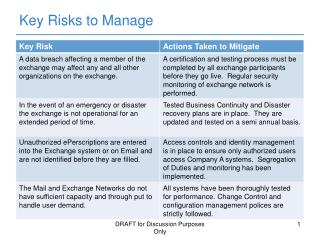
Empirical Test of Full Insurance Effect of Health Expenditures on Per Capita Non-Medical Consumption Robust standard errors in parentheses, clustered by strata *** p<0.01, ** p<0.05, * p<0.1 Insurance in Combination with Other Financial Services
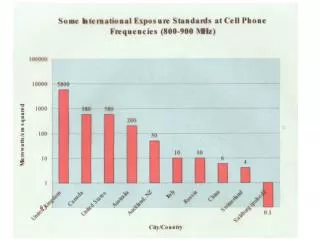
Theory of Insurance • Households should be willing pay a “risk premium” in excess of expected expenses to insure against illness • Based on variance of losses, income & risk tolerance: • Use TLSS to estimate maximum % of expected benefits that households would pay to fully insure ambulatory medical care • Typically lower for outpatient care than for hospitalization due to lower variance (Pauly, Blavin, & Meghan, 2010) • Compare to plausible levels of administrative loading • ~30% in other developing countries • Higher regulatory & monitoring costs for informal payments to public providers • Higher loading costs for outpatient care given greater number of transactions & providers • Also aggravates selection problem (especially with relatively low risk aversion) Insurance in Combination with Other Financial Services
Estimated Demand for Insurance Survey-Adjusted Risk Premium (2007/2009 Panel) * CRRA Insurance in Combination with Other Financial Services
Policy Implications • Do outpatient medical expenditures affect household consumption? • TLSS data suggests health expenditures are only partially offset through informal coping mechanisms & negatively affects current consumption • More pronounced among the poorest households • Is there demand for insurance and/or precautionary savings for health? • Absence of insurance for ambulatory care appears consistent with low demand relative to plausible loading • Variance of OOP spending still high enough to affect behavior & policy → suggests high value of savings & other mechanisms to smooth consumption more cheaply • Consistent with observed demand for health savings in India, Kenya & Burkina Faso • Potential for bundling with hospitalization insurance • Why don’t the poor currently save enough for that purpose? • Inefficient capital markets combined with biased beliefs, inattention, inconsistent preference & other behavioral constraints Insurance in Combination with Other Financial Services
Future Research • Would savings increase utilization and/or out-of-pocket health spending? • Depends on demand elasticity & price discrimination • Preliminary evidence from recent pilots & objective of future research • Do savings actually improve health outcomes? • Unknown →mitigated by poor treatment-seeking behaviors on the part of patients combined with low quality & corruption on the part of providers • More ambiguous demand function (price elasticity & non-price factors), combined with less obvious outpatient health benefits • Need for patient education plus incentives for high-quality care & evidence-based treatment Insurance in Combination with Other Financial Services