Download
1 / 45
610 likes | 1.17k Views
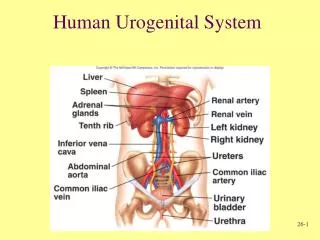
DEVELOPMENT OF UROGENITAL SYSTEM. By Dr Samina Anjum. PHYLOGENETIC STAGES. Pronephros, a structure similar to that found in primitive vertebrates. Mesonephros , a more advanced system found in fish & amphibia. Metanephros which elaborates into the final human form.

E N D
DEVELOPMENT OF UROGENITALSYSTEM By Dr Samina Anjum
PHYLOGENETIC STAGES • Pronephros, a structure similar to that found in primitive vertebrates. • Mesonephros, a more advanced system found in fish & amphibia. • Metanephros which elaborates into the final human form.
DEVELOPMENT OF 3 SETS OF OVERLAPPING KIDNEY SYSTEMS IN CRANIOCAUDAL SEQUENCE
PRONEPHROS (EARLY 4th WEEK) • Rudimentary, transitory and non functional • Represented by 7 to 10 solid cell groups in cervical region • These groups form vestigial excretory units, nephrotomes • Pronephric duct runs caudally and opens into cloaca
PRONEPHROS • Cranial segments regress before more caudal ones are formed • End of 4 wks - Disappears
MESONEPHROS/ INTERIM KIDNEYS FUNCTION FOR 4 WKS The Mesonephros and ducts are derived from intermediate mesoderm of upper thoracic to upper Lumber L3 segments. Functional for a short time during early fetal period
Early in 4th week the first excretory tubules of mesonephros appear, during regression of pronephric system • Formation of S- shaped excretory tubules & glomerulus • Formation of Bowman's capsule • Renal corpuscle • Laterally the tubules enter into mesonephric/ Wolffian duct, a continuation of the pronephric duct
IN THE MIDDLE OF SECOND MONTH • Mesonephros forms large ovoid organon each side of midline. • Gonad develops on the medial side of urogenital ridge
BY THE END OF SECOND MONTH: • While caudal tubules are still differentiating, cranial tubules & glomeruli show degenerative changes • Mesonephric duct opens into cloaca • In males a few caudal tubules and the mesonephric duct persist and participate in formation of genital system, but disappear in female
METANEPHROS/DEFINITIVE/PERMANENT KIDNEY • Appears in 5th wk • Permanent kidney develops from two sources: • Metanephric diverticulum / Ureteric bud give rise to collecting system • Metanephric mesoderm/ blastema give rise to excretory units
COLLECTING SYSTEM • Collecting ducts develops from ureteric bud as an out growth of mesonephric duct • The ureteric bud penetrates the metanephric tissue which is moulded over its distal end as a cap.
Cont… • The ureteric bud penetrates the metanephric tissue which is moulded over its distal end as a cap. • The ureteric bud will grow into, and branch several times within, the metanephric mesenchyme, like a plant root penetrating and growing within ground soil.
The distal end of bud dilates forming the renal pelvis and splits into cranial and caudal portions, major calyces • Each calyx will form two new buds while penetrating into the metanephric mesoderm. These buds continue to subdivide until 12 or more generations of tubules formed
Cont… • The tubules of 2nd order enlarge and absorb those of 3rd and 4th generations, forming the minor calyces of renal pelvis. • During further development collecting tubules of 5th and successive generations elongate considerably and converge on the minor calyx, forming the renal pyramid.
DERIVATIVES OF METANEPHROS • Metanephric diverticulum / Ureteric bud: • Ureters • Renal pelvis • Calyces • Collecting tubules (1-3 million) • Metanephric blastema • Bowman’s capsule • PCT • Loop of Henle • DCT
Nephrons are formed until birth, at which time there are 1 million nephrons in each kidney. • Urine formation by 10th week • At birth, kidneys have a lobulated appearance, but the lobulation disappears during infancy as a result of further growth of nephrons, although no increase in their number
REGULATION OF KIDNEY DEVELOPMENT • The ureteric bud is essential for induction of differentiation in the metanephric mesoderm. • The metanephric cap is essential for bifurcation of the ureteric bud. • The collecting ducts are essential for differentiation of the nephrons.
POSITION OF KIDNEY Initially in the pelvic region, later shifts to a more cranial region in the abdomen. Attain adult position by the 9 weeks This ascent of kidney is caused by: • Diminution of body curvature • Growth of body in lumber and sacral regions (abdomen and pelvis)
HILUM OF KIDNEY • Faces ventrally initially; but as the kidney ascends, it rotates medially almost 90 degrees. By the 9th week the hilum is directed anteromedially. Eventually the kidneys become retroperitoneal on the posterior abdominal wall.
CHANGES IN BLOOD SUPPLY OF KIDNEYS • In the pelvis metanephros receives its arterial supply from pelvic branch of aorta. • During its ascent to the abdominal level, it is vascularized by the arteries that originate from aorta at continuously higher levels. • Lower vessels usually degenerate • Accessory renal arteries
FUNCTION OF KIDNEY • The definitive kidney becomes functional by 12th week • Urine is passed into amniotic cavity and mixes with amniotic fluid • Fluid is swallowed by the fetus and recycles through the kidneys • During fetal life kidneys are not responsible for excretion of waste products
The kidneys and suprarenal glands of 28 weeks fetus. The external evidence of the lobes usually disappears by the end of first year.
ABNORMAL LOCATION OF THE KIDNEY • Pelvic kidney--- if fails to pass through arterial fork formed by umbilical arteries. Remains in the pelvis close to common iliac artery
Horse shoe kidney in a 13 wk female fetus In 1/600 people kidneys are pushed so close together during their passage through the arterial fork that the lower poles fuse. The large U-shaped kidney usually lies in the hypogastrium, anterior to the inferior lumbar vertebrae. Normal ascent of these fused kidneys is prevented because they are caught by the root of the inferior mesenteric artery. A horseshoe kidney usually produces no symptoms because its collecting system develops normally and the ureters that arise from anterior surface of kidney enter the bladder normally.
WILM’S TUMOR • Is a cancer of kidney that usually affects children by 5 years of age. • Many are now known to be associated with genetic defects (WT1 genes on chromosome 11). • May be associated with other abnormalities and syndromes e.g. WAGR syndrome, Denys – Drash syndrome. • Nowadays, treatment gives a better than 90% --- 5 year survival. Small kidney from a 4 year old child contains a lobulated tan-white mass (Wilms tumor of the kidney).
RENAL DYSPLASIAS AND AGENESIS • Spectrum of severe malformations that represent the primary diseases requiring dialysis and transplantation in the 1st years of life • In unilateral agenesis the other kidney usually undergoes compensatory hypertrophy and performs the function of missing kidney
RENAL AGENESIS • May arise if the interaction between the metanephric mesoderm and the ureteric bud fails to occur. Reason: Genes Mutations • Bilateral renal agenesis is usually associated with oligohydroamnios because little or no urine is excreted into the amniotic cavity
AUTOSOMAL RECESSIVE POLYCYSTIC KIDNEY DISEASE • Occurs in 1/5,000 births • A progressive disorder in which cysts form from collecting ducts. • The kidneys become very large and contain many hundreds of small cysts. Renal failure occurs in infancy or childhood • Survival depends upon postnatal dialysis and kidney transplantation
AUTOSOMAL DOMINANT POLYCYSTIC KIDNEY DISEASE • Cysts form from all segments of the nephron and usually do not cause renal failure until adulthood. • More common (1/500 or 1/1,000 births) but less progressive than the autosomal recessive disease
DUPLICATION OF THE URETER • Results from early splitting of ureteric bud • Complete or Partial • Ectopic ureter
DEVELOPMENT OF URINARY BLADDER • During 4th to 7th week of development, the cloaca divides into UROGENITAL SINUS anteriorly & the anal canal posteriorly • Urorectal septum: the tip will form the perineal body
Three portions of urogenital sinus are: • Upper & largest part • Pelvic part • Phallic part: as genital tubercles grow this part is pulled ventrally A thick fibrous cord
Median umbilical ligament 18 wk fetus
During differentiation of cloaca, the caudal portions of mesonephric ducts are absorbed into the wall of urinary bladder to form the Trigone • Mesonephric ducts move close together to enter the prostatic urethra and in the male become the ejaculatory ducts • With time the mesodermal epithelium of trigone changes & is replaced by endodermal epithelium
DEVELOPMENT OF URETHRA • Origin of epithelium in both sexes --- endoderm • Surrounding C.T. and smooth muscle --- splanchnic mesoderm • At the end of 3rd month, epithelium of prostatic urethra begins to proliferate and forms a number of outgrowths that penetrate the surrounding mesenchyme.
In the male, these buds form the PROSTATE GLAND • In the female, the cranial part of urethra gives rise to the URETHRAL AND PARAURETHRAL GLANDS
BLADDER DEFECTS • URACHAL FISTULA • URACHAL CYST • URACHAL SINUS
EXSTPROPHY OF BLADDER • Ventral body wall defect • Epispadias is a constant feature and open urinary tract extends up to umbilicus • Is due to the failure of lateral body wall folds to close in the midline in the pelvic region • This anomaly is rare, occurring in 2/100,000 live births
EXSTROPHY OF CLOACA • More severe ventral body wall defect • Progression and closure of lateral body folds are disrupted to a greater degree • The defect involves both the anterior abdominal wall and the anterior wall of urinary bladder • Normal development of urorectal septum is altered resulting in other defects like: • Imperforate anus • Other anal canal malformations • Defects in external genitalia • Occurrence is rare i.e. 1/30,000 births