Download
1 / 49
660 likes | 1.88k Views
ALLERGIC CONJUNCTIVITIS. Nazri Omar, MD, PhD Consultant ophthalmologist Department of Surgery Faculty of Medicine & Health Sciences, Universiti Putra Malaysia. What is it?.

E N D
ALLERGIC CONJUNCTIVITIS Nazri Omar, MD, PhD Consultant ophthalmologist Department of Surgery Faculty of Medicine & Health Sciences, Universiti Putra Malaysia
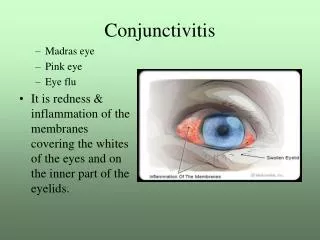
What is it? • Is an inflammation of the conjunctiva, the mucous membrane lining the anterior sclera and inner eyelid surfaces in response to an allergen either persistent (house dust, mite) or transient (pollen).
Cross section of the eye showing regions commonly involved in allergic reactions
Hypersensitivity Reaction • Type I (immediate) • Type II • Type III • Type IV (delayed type)
Types of allergic conjunctivitis • Seasonal Allergic Conjunctivitis (SAC) • Perennial Allergic Conjunctivitis (PAC) • Vernal Keratoconjunctivitis (VKC) • Atopic Keratoconjunctivitis (AKC) • Giant Papillary Conjunctivitis (GPC)
Acute allergic rhinoconjunctivitis • Most common form of ocular and nasal allergy • Hypersensitivity reaction to specific airborne antigens. • Classification : 1. Seasonal allergic rhinoconjunctivitis - with onset of ‘hay fever’ during summer - commonest and mildest form of allergic
Cont. - conjunctivitis. - allergens : pollens 2. Perennial allergic rhinoconjunctivitis - symptom throughout the year, exacerbation autumn - less prevalent and milder than seasonal, but more persistent - allergens : dust mites and fungal
Cont. • Presentation • transient, acute attacks of redness, watering and icthing a/w sneezing and nasal discharge. • Signs • lid oedema • conjunctiva has a milky or pinkish appearance as a result of oedema and injection. • small papillae on the upper tarsal conjunctiva • Treatment
Seasonal allergic conjunctivitis. Perennial allergic conjunctivitis (PAC)
Vernal Keratoconjunctivitis • Recurrent, bilateral, external, ocular inflammation • Affecting boys and young adults living in warm, dry climates • IgE and cell-mediated immune mechanisms • 75% - associated atopy • 67% - family history of atopy
VKC • Often develop asthma and eczema in infancy • Onset usually after age of 5 years, and eventually resolves around puberty • May occur on seasonal basis, but many patients have year round disease. • Higher incidence of keratoconus
VKC • Presentation • intense ocular icthing a/w lacrimation, photophobia, foreign body sensation and burning • thick mucus discharge and ptosis also occur • Three main clinical types • (a) palpebral • (b) limbal • (c) mixed
VKC - Clinical features 1. Palpebral VKC • diffuse papillary hypertrophy, most marked on superior tarsus • papillae enlarge and have a flat-topped polygonal appearance • cobblestones • severe cases : giant papillae, may be coated by copious mucus 2. Limbal VKC • mucoid nodules scattered around the limbus with discrete white superficial spots (Horner-Trantas dots) • collection of eosinophils at the apices of the lesions
Large papillae on the upper tarsus in vernal keratoconjunctivitis. Horner-Trantas dots at the superior limbus in vernal keratoconjunctivitis.
VKC – Clinical features • Keratopathy • Punctate epithelial erosions • Superior cornea • Shield ulceration • may be complicated by bacterial keratitis and rarely perforation
Upper tarsal surface in vernal keratoconjunctivitis showing ‘cobblestone’ appearance. Punctate Epithelial Erosions
A corneal shield ulcer in vernal keratoconjunctivitis. Vernal keratoconjunctivitis - a more chronic form of ocular allergy.
VKC 3. Plaque formation • base of the ulcer coated with dessicated mucus. • defective wetting by tears, prevents reepithelialization then predisposes to subepithelial scarring and vascularization. 4. Pseudogerontoxon • resembles an arcus senilis • ‘cupid’s bow’ outline in a previously inflamed segment of the limbus
VKC • Treatment 1. Topical (i)Steroids indicated for keratopathy eg. Fluorometholone (ii)Mast cell stabilizers – prophylactic theraphy eg. Nedocromil bd, Iodoxamide qid
VKC (iii)Antihistamines – eg. levocabastine (iv)Acetylcysteine 0.5% - mucolytic properties, useful in treatment of early plaque formation (v)Cyclosporin 2% - useful in steroid-resistant cases 2. Supratarsal steroid injection - Betamethasone or triamcinolone - patient with severe disease, unresponsive to conventional therapy
VKC 3. Surgical - debridement, superficial keratectomy, excimer laser phototherapeutic keratectomy and amniotic membrane transplantation - may required for severe shield ulcers resistant to medical therapy
Atopic Keratoconjunctivitis • Rare but potentially serious condition • Young men with atopic dermatitis • May persists for many years • High rate of significant visual morbidity • May develop visual impairment from keratoconus, presenile cataract and rarely retinal detachment
Posterior subcapsular cataract associated with steroid use.
AKC • Clinical features 1. Eyelids • red, thickened, macerated and fissured • associated chronic staphylococcal blepharitis 2. Conjunctivitis • inferior forniceal and tarsal conjunctiva • pale and featureless appearance • exacerbations : chemosis, limbal hyperaemia and papillary hypertrophy • advanced cases : cicatrizing conjunctivitis may develop with inferior forniceal shortening and symblepharon formation
AKC 3. Keratopathy • Punctate epithelial erosions • persistent epithelial defects • shield-shaped anterior stromal scars • peripheral vascularization 4. Complications • herpes simplex keratitis and microbial keratitis
AKC - treatment (i) lid hygiene - asso. Staphylococcal blepharitis (ii) Preservatives-free lubricants (iii) Steroids – short term • severe inflammatory exacerbations and keratopathy (iv)Mast cell stabilizers – eg. Sodium cromoglycate, nedocromil and lodoxamide
AKC - used throughout the year as prophylaxis (v)Non-steroidal anti-inflammatory agents - eg. Ketorolac (vi)Antihistamines (vii)Cyclosporin 2% 2. Supratarsal steroid injection - when topical treatment is ineffective
AKC 3. Systemic (a)Antihistamines – useful in severe itching (b)Antibiotics – eg. Azithromycin 500 mg od for 3 days - effective in reducing inflammation aggravated by staphylococci (c)Cyclosporin – severe cases
Staphylococcal blepharitis with hyperemic eyelid margins and crusts. Trichiasis and madarosis are also present. Staphylococcal blepharitis with inflamed lash follicles.
Atopic keratoconjunctivitis with conjunctival papillae in the left image and conjunctival cicatricial changes in the right image. Atopic keratoconjunctivitis with symblepharon. The eyelids in atopic keratoconjunctivitis.
Giant Papillary Conjunctivitis • Immune-mediated inflammatory disorder • Causes - irritation of superior palpebral conjunctiva • Poorly fitting contact lens, ocular prostheses or exposed sutures • Allergy to lens material • Immunological reaction to contact lens deposits
GPC • Presentation - months or years after exposed - ocular itching, increased mucus production in the morning, photophobia and decreased lens tolerance - blurred vision sometimes • Signs - spectrum of changes on the upper tarsal
GPC conjunctiva : mild papillary response full-blown picture of GPC (giant papillae >0.3 mm) - excessive mucus in the eye and on the contact lens - Trantas’ dots, limbitis and peripheral corneal infiltration - mechanical ptosis in severe cases
GPC - treament • optimized lens hygiene • adjustment of lens fitting • change in lens type • topical treatment with mast cell stabilizer • avoid long term steroids
Medication • Antihistamine (topical/systemic) • Mast cell stabilizer • Steroids (topical/systemic) • Non-steroidal anti-inflammatory drug (NSAID) • Lubricating eye drops • Cyclosporin • Mucolytic agent
Antihistamine • Block histamine receptors at H1 and H2 • Relieve acute symptoms (itching, redness) • Eg. Emedastine difumarate (Emadine) Levocabastine (Livostin) Epinastine (Elestat) Azelastine (Optivar) • Side effect (systemic) : drowsiness, dry mouth
Mast cell stabilizers • Aid in the phosphorylation of a protein that terminates secretion of mast cells granules • Increased calcium influx into the cells preventing membrane changes • Reduce membrane fluidity prior to mast cell degranulation
Cont. • Prevents release of histamine and other chemotactic factors • Eg. Sodium cromoglycate (Opticrom) Lodoxamide tromethamine (Alomide) Olopatadine (Patanol) Ketotifen (Zaditor) Nedocromil (Alocril) • Side effects : ocular irritation, headache, nasal congestion and unpleasant taste
Cont. • Do not relieve existing symptom • As prophylactic basis
Steroids • Act on arachidonic acid pathway • Inhibiting phospholipase responsible for converting major phospholipid into arachidonic acid • Preventing formation of arachidonic acid • Thus block both cyclooxygenase and lipoxygenase pathway
Cont. • Eg. Fluorometholone (FML) Rimexolone Medrysone Prednisolone acetate Lotemax 0.05% Alrex 0.02% • Side effects : delayed wound healing, secondary infection,
Cont. elevated IOP and formation of cataract • Presribed at the lowest effective concentration and for shortest duration • Pulse-therapy regimen
NSAIDs • Act on cyclooxygenase metabolic pathway • Inhibits production of prostaglandin and thromboxanes • Eg. Ketorolac tromethamine (Acular) • Side effects : corneal deposits, diminished vision, retinal disturbances, scotomata and changes in colour vision
Lubricating Agent • Help to improve the first-line defense at the level of conjunctival mucosa • Dilute various allergens and inflammatory mediators and flush them from ocular surface • Eg. Artificial tears (preservatives free) if available
Cyclosporin • Inhibition of ability of T-lymphocyte to produce interleukin 2 (IL-2) • Thus inhibition for recruiting and activating new T cells • Eg. Restasis (CSA 0.05%)