Download
1 / 16
200 likes | 1.79k Views
Neontal Conjunctivitis. Patricia Wang, R1 11/5/13. Neonatal Conjunctivitis. Septic Bacterial Viral Aseptic Most often chemical conjunctivitis. Anatomy of conjunctiva. Thin translucent mucous membrane Nonkeratinizing, squamous epithelium and a thin, richly vascularized stroma

E N D
Neontal Conjunctivitis Patricia Wang, R1 11/5/13
Neonatal Conjunctivitis • Septic • Bacterial • Viral • Aseptic • Most often chemical conjunctivitis
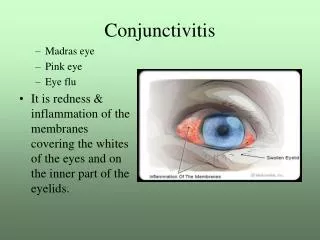
Anatomy of conjunctiva • Thin translucent mucous membrane • Nonkeratinizing, squamous epithelium and a thin, richly vascularized stroma • Has accessory lacrimal glands and goblet cells • Conjunctiva inflammation can cause blood vessel dilation, swelling, and excessive secretions
Gonococcal Conjunctivitis • More virulent • Infection • Typically acquired during passage through birth canal • Can have intrauterine infection after ROM • Clinical features • Bilateral purulent conjunctivitis • Chemosis and eyelid swelling • Can extend deeper • Leads to corneal ulceration, scarring, perforation and visual impairment • May have systemic manifestations • Diagnosis • Culture on chocolate agar and/or Thayer-Martin • Treatment • Treat until culture results • Ceftriaxone (25–50 mg/kg, intravenously or intramuscularly, not to exceed 125 mg)
Chlamydial conjunctivitis • Obligate intracellular parasite • Most common infectious cause • Via passage through birth canal • High transmission • May have intrauterine transmission • Later onset • Usually starts 5 to 14 days after delivery • Earlier in infants born to mothers with PROM • Clinical presentation • Mild and self-limited • Unilateral or bilateral • Presents with watery discharge that can progress to mucopurulent discharge • Can have eyelid edema, pannus and/or pseudomembrane formation • Concomitant infection • Nasopharynx, lungs, and/or genital tract
Chlamydial Conjunctivitis • Diagnosis • In past, basophilic intracytoplasmic inclusion bodies from a conjunctival scraping with Giemsa stain or culture • Via PCR • Increased sensitivity, same specificity as culture • Treatment • Systemic • PO erythromycin (50 mg/kg/d divided qid) x 14 d
Other bacterial conjunctivitis • Make up 30-50% of all cases • Staph aureus, Strep pneumo, Strep viridans, and Staph epi • Gram-negative organisms • E coli, Kleb pneumo, Serratia marcescens, and Proteus, Enterobacter, and Pseudomonas • Low birth weight and low gestational age
Neonatal HSV • Usually presents 6 to 14 days after birth • Via birth • Consider C-section if active lesions • Clinical presentation • May only be eye infection • Can have herpetic vesicles on eyelid margins, but often absent • Microdendrites or geographic ulcers • Eyelid edema, conjunctival injection, and serosanguineous discharge
Neonatal HSV • Diagnosis • Via conjunctival or corneal cultures • May be delayed • May require ophthalmology consult for definitive diagnosis and management • Should be admitted to evaluate of disseminated and CNS herpes infection • Treatment • IV acyclovir (60 mg/kg per day in three divided doses for 14-21 days) and topical antiviral therapy (eg, trifluridine drops)
Prophylactic ophthalmic antibiotics • Drastically reduces risks of conjunctivitis • AAP and CDC recommend • 0.5% erythromycin ointment (1 cm ribbon in each eye) • 1% tetracycline ointment (1 cm ribbon in each eye) • Alternatives include azithromycin, gentamicin, or tobramycinophthalmic ointment • No efficacy performed on alternatives • Should examine closely • Not as effective in preventing neonatal chlamydial conjunctivitis • Povidone-iodine more effective against C. trachomatis
Infants with a potentially sexually transmitted disease should undergo evaluation for other sexually transmitted diseasesas should the mother and her sexual partner
Application of prophylaxis • Place in lower conjunctival sacs • Spread by gentle massage of eyelids • Can wipe extra away after 1 min • Don’t irrigate after application, can reduce efficacy • Should be within the first hour of life in all infants, regardless of vaginal or cesarean section • Efficacy of longer delays not known • Side effect chemical (noninfectious) conjunctivitis • More common with silver nitrate
Chemical conjunctivitis • Can be caused by silver nitrate drops • Usually begins a few hours after administration • Lasts about 2-3 days • ~90% infants that receive silver nitrate develop mild, transient conjunctival injection with excessive tearing • Can damage corneal epithelium • Not used as ocular prophylaxis postpartum in US
Resources • Uptodate, neonatal conjunctivitis • AAP • Red Book