Download

1 / 33
330 likes | 453 Views
The Medical Home Model: Case Management Perspectives. James W. Mold, MD, MPH Department of Family and Preventive Medicine University of Oklahoma HSC-OKC. Disclosures. To my knowledge I have no conflicts of interest. I won’t mention any specific companies or products in my presentation.

E N D
The Medical Home Model: Case Management Perspectives James W. Mold, MD, MPH Department of Family and Preventive Medicine University of Oklahoma HSC-OKC
Disclosures • To my knowledge I have no conflicts of interest. • I won’t mention any specific companies or products in my presentation. • I am a family physician with additional trainingin geriatrics and I bring those biases with me.
Learning Objectives By the time I have finished, you should be able to: • Define the Patient-Centered Medical Home (PCMH) • Explain the relationship between the PCMH and the Chronic Care Model • Summarize the conditions under which case management has been found to be effective in primary care settings • Explain differences between a disease-oriented approach and a patient-oriented approach to care
Outline • Definitions and conceptual models • Primary care • Chronic Care Model (CCM) • Patient-Centered Medical Home (PCMH) • Case management in primary care • Evidence review • Implications • Patient-centeredness and its implications • Goal-orientation vs. disease orientation • Case management in rural America • County health improvement organizations
Primary Care • The Institute of Medicine, in 1996, defined primary care as “the provision of integrated, accessible, health-care services by clinicians that are accountable for addressing a large majority of personal health-care needs, developing a sustained partnership with patients, and practicing within the context of family and community.” • Attributes Accessible Family-centered Comprehensive Community-centered Coordinated Relationship-Based Longitudinal Integrated Person-centered
Primary Care Organizational AttributesIntegrated • Accessible • Comprehensive • Coordinated • Longitudinal Clinical AttributesIntegrated • Person-centered • Family-centered • Community-centered • Relationship-Based
Impact of the CCM on Primary Care • Information systems • Electronic health records (EHRs) • Health information exchange (HIE) • Registries for population management • Decision support • Guidelines • Prompt/reminder systems, dashboards, protocols, checklists • Delivery system design • Teamwork • Standardized consultations • (Concierge practices) • Patient self-management support
Patient Self-Management Support • Patient education • One-on-one • DVDs • Bibliotherapy • Training for monitoring health parameters • Action plans (what to do, who and when to call) • Monthly phone contacts • Connections • Community resources • Support groups • Reminders and incentives to make positive behavior changes
Examples • Diabetes • Diabetes education • Q3month visits • ADA Guideline-based protocols, flow sheet • Single eye consultant • Registry • Prenatal care • Prenatal classes • Scheduled visits • ACOG Guidelines, flow sheet • High-risk OB clinic • Due date registry
Impact on Primary Care • Applicable to prevention as well as chronic illness care • CCM now often referred to as the Care Model • Enhancement of comprehensiveness, coordination and longitudinality • Emphasis on diseases and guidelines could threaten person-centeredness, relationship-based care • Industrial quality model (every widget the same) • Would require an additional 3.5 to 10.6 hours per day for 10 most common chronic diseases. Ostbye T et al. Ann Fam Med 2005; 3(3): 209-214.
Impact on Primary Care Creates need/increased opportunities for: • Health educators • Case managers • Panel managers, registry managers • Social workers • Patient coaches • Patient navigators • Community health workers • Practice – Community Connectors
Patient-Centered Medical Home (PCMH) “A patient-centered medical home integrates patients as active participants in their own health and well-being. Patients are cared for by a physician who leads the medical team that coordinates all aspects of preventive, acute and chronic needs of patients using the best available evidence and appropriate technology. These relationships offer patients comfort, convenience, and optimal health throughout their lifetimes.” American Academy of Family Physicians, the American Academy of Pediatrics, and the American College of Physicians Spring, 2008.
PCMH as Advanced Primary Care Primary care that incorporates the CCM while preserving (enhancing) person-centeredness and adding HIT and QI • Increased emphasis on access and convenience • Open access scheduling • Extended hours • Incorporation of new technologies • Electronic health records, health information exchnage • Personal health records • Patient portals and E-visits • Quality Monitoring • Disease-oriented or standardized preventive services • Patient satisfaction
PCHMH Standards • NCQA criteria look like CCM plus e-prescribing, test tracking, referral tracking, and continuous quality improvement • “Care management” is one of nine sections • AAFP/TransforMed criteria look like primary care plus continuous quality improvement • Case management not specifically listed • OK SoonerCare criteria emphasize care management; 3 tiers • Other criteria: AAAMC, The Joint Commission, the Center for Medical Home Improvement, BCBS of Michigan, Minnesota’s Health Care Home Certification Program
PCMH Standards Care Coordination Population Management Care Plan Health IT Team-Based Care Evidence-Based Care Etc. Burton RA, et al. Report to CMS by the Urban Institute, May, 2011
Case Management Case Management is a collaborative process that promotes quality care, and cost effective outcomes which enhance the physical, psychosocial and vocational health of individuals. It includes assessing, planning, implementing, coordinating, and evaluating health related service options.
Case Management in Primary Care What we now know: • Case managers must interact with patients in person; not just by phone Ayanian JZ. JAMA 2009; 301(6): 668-670 • Case management must be integrated into primary care Seow H, et al. JAGS 2006; 54:535-540 Wolff JL, et al. Ann Intern Med 2005; 143(6): 439-445 • A disease-oriented, guideline-driven approach is probably less effective than a patient-centered, goal-directed approach Congressional Budget Office Analysis, 2004 Bosmans J, et al. J Gen Intern Med 2006; 21: 1020-1026 • Patient selection is important, but the best approach isn’t clear yet
Primary Care Organizational AttributesIntegrated • Accessible • Comprehensive • Coordinated • Longitudinal Clinical AttributesIntegrated • Person-centered • Family-centered • Community-centered • Relationship-Based
Case Management in the PCMH • Organizational Integration • Access process • Same office • Same record • Unified assessment • Effective and efficient communication channels • Clinical Integration • Person-centered • Goal-directed • Relationship-based • Context-sensitive
Case Management in the PCMH • Access options • Disease-based (CHF, DM, asthma, etc.) • Risk projections (computer formulas) • Internal referrals (from primary care clinicians) • Patient self-referrals (e.g. availability advertised) • CM self-referrals (e.g. all patient’s screened) • Combinations of above options • Transitions between care settings also very important • Hospital to home • Home to AL, NH • Home to ED to home
Case Management in the PCMH • Same Office • “I’m calling from Dr Smith’s office. He wanted me to visit with you about…” • Same record • CM notes in same section as physician notes • Unified assessment • CM begins with information already in record. • Additional information is added to appropriate sections of the record. • Communication channels • EHR messaging, daily event reports • Hallway huddles • Weekly team meetings? • Care plan visits (clinician, patient, family, CM)?
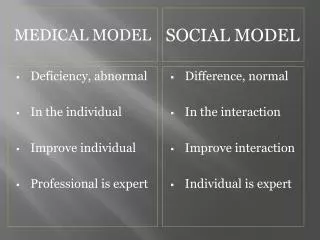
Case Management in the PCMH • Person-centered • Primary focus is on the needs of the person, not on management of their diseases (though that too) • Goal-directed • A goal is a desired outcome for which it makes little sense to say, “…so that?” I’d like to live long enough to see my grandchild get married. I’d like to get be able to use mysewing machine again. Not, “I’d like to get my A1c to <8%.” • Relationship-based • Human interpersonal interactions my be the most powerful therapeutic agents in our armamentarium.
Practical Considerations • Who can/should do it? • Children mostly need a social worker • Old people mostly need a skilled nurse • Some combination of these might be ideal • How many case managers are needed? • Assistive care management to address adherence problems, complex medication regimens, and co-morbidities for the 20 percent to 30 percent of patients whose diseases are not under control. • Intensive case management and specialty care for the 1 percent to 5 percent of patients with advanced disease and complex co-morbidities or frailty. • How should it be organized and financed? • Reimbursement to practices (fee-for-service) • Capitation payment to practice • Support for a set of shared resources
Bodenheimer T, et al. JAMA 2002; 288(14): 1775-1779 and 288(15): 1909-1914.
NC Community Care • 14 non-profit networks covering the entire state • NC Medicaid puts $3 PMPM into the networks and gives primary care clinicians $2 PMPM to join a network • Networks use the money to hire or contract for case managers and others needed to improve care and reduce cost • QI projects initially directed by the state (CHF, DM, asthma) • Networks now encouraged to initiate QI projects • Successful projects spread to other networks • Extremely successful in terms of cost savings, improved quality measures, and better relations (PCC and Medicaid)
OK Health Access Networks • 3 non-profit HANs (Canadian County, OU-Tulsa, OSU COM) • Medicaid puts $5 PMPM into the networks • Networks hire or contract for case managers • Required to help practices reach level 3 PCMH • Some empahsis on HIT and HIE • Too early to tell if effective
Effective Implementation of Innovations in Primary Care Literature and Exemplar Methods Academic Detailing Performance Feedback Facilitation Practice Enhancement Assistant IT Support Local Learning Collaboratives
Primary Care Mental Health Public Health Practice OHIET Regional AHEC Practice Practice County Health Improvement Office QI Facilitators Case Managers IT Support Practice Practice Practice Academic Medical Centers Funders Turning Point Hospital
OHIET NW AHEC SW AHEC NE AHEC SE AHEC P P P P CHIO P CHIO CHIO CHIO CHIO CHIO CHIO CHIO P P P P P P CHIO P P P P CHIO P CHIO CHIO P P P P P P OUHSC OKC OSU-COM OU-CCM Tulsa
Annual Funding Public and Private Insurers Project Specific Funding AHRQ, NIH, etc. Medical Centers Oklahoma Health Information Exchange Trust OSDH,OPCA,OFMQ Regional AHECs Project Specific Funding CDC, HRSA, etc. County Extension Program County Extension Program County Extension Program County Extension Program State, Local, Private Funding??
Learning Objectives By the time I have finished, you should be able to: • Define the Patient-Centered Medical Home (PCMH) • Explain the relationship between the PCMH and the Chronic Care Model • Summarize the conditions under which case management has been found to be effective in primary care settings • Explain differences between a disease-oriented approach and a patient-oriented approach