Download
1 / 43
430 likes | 545 Views
Page What is IVF 3 Medication Suppression 5 Stimulation 10 Prepare for Retrieval 11 Post operative 12 Administration SC injections 14 IM injections 15 Monitoring 16 Daily Cycle Instructions 21 Preoperative appointment 22. Page Day of egg retrieval 23

E N D
Page What is IVF 3 Medication Suppression 5 Stimulation 10 Prepare for Retrieval 11 Post operative 12 Administration SC injections 14 IM injections 15 Monitoring 16 Daily Cycle Instructions 21 Preoperative appointment 22 Page Day of egg retrieval 23 Sperm collection 25 Day after egg retrieval 28 Day of embryo transfer 29 Cycle Cancellation 31 Complications 32 Embryo Freezing 33 Pregnancy test 34 Emergencies 35 Typical Cycle 36 Consents 37 Nurse Appointment 38 Table of ContentsClick on an item below to go directly to that page. Once there, hit the arrow on the page to get back to the Table of Contents.
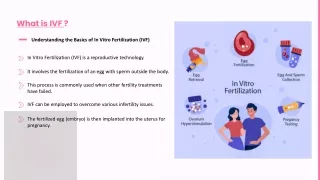
What is IVF? • Stimulate the ovaries to mature many eggs • Surgically remove eggs • Mix with sperm • Incubate fertilized eggs • Return a few to the uterus
What is IVF? • Starts the month before the stimulation • Lasts approximately 8 weeks • Medication for about 6 weeks • To start, call your nurse with your period
Medications • Suppression Medicines • Begin the month before the stimulation • Birth Control pills • Lupron • Ganirelix • Cetrotide • Climera patch
Medications • Suppression Medicine • Birth control pills • Start d1-3 • Suppress LH & FSH hormones • Regulate cycles, active pills only • Side effects • Early pregnancy symptoms • Breakthrough bleeding
Medications • Suppression Medicine • Lupron • Suppress LH, FSH, estrogen, and progesterone • Better quality eggs • Stops ovulation • Once or twice a day injection • Side effects: hot flashes, insomnia, headache • Use condoms • Allergy: local redness
Medications • Suppression Medicine • Ganarelix/Cetrotide • Suppress LH immediately • Once a day injection • Fewer shots • Side Effects: headache, nausea
Medications • Suppression Medicine • Climera patch • Stabilizes and thickens the uterine lining • Skin patch placed anywhere except the chest • Changed every other day • Side effects: headaches, breast tenderness, uterine cramping and bloating. Rare: blood clots
Medications • Stimulation Medicine • Gonal-F, Follistim, Bravelle Repronex, Menopur • Mature many eggs at once • Once or twice a day injection • Side Effects/risks: • Mood swings • Bloating • Ovarian hyperstimulation
Medications • Preparation for Retrieval • HCG, Pregnyl, Novarel • Final maturing of eggs • Given: • 4 follicles (2 follicles with mean ≥17-18mm) • Estradiol level is at least 600 • 36 hours before egg retrieval Risk: early ovulation, OHSS
Medications • Post Retrieval Medicine • Progesterone • Supports the lining of the uterus • Injectable, vaginal suppository, vaginal gel • May delay period • Continue even if bleeding starts • Side effects similar to pregnancy
Medications • Post Retrieval Medicine Doxycycline - antibiotic • All patients • Pills • Estrace – Estrogen • ICSI, AH, PGD patients • Pills • Medrol- anti-inflammatory • ICSI, AH, PGD patients • Pills
Medication Administration Subcutaneous (small needle) injection Clean the injection site with an alcohol wipe by rubbing in a circular motion. Remove the needle cap. Pinch the injection site with one hand. Using the other hand, quickly insert the needle straight in as far as it will go. Inject the medication by pushing the plunger down to empty the syringe. Remove the needle. Rub the area in a circular motion to massage the medication. Dispose of the syringe in a “sharps” container. If you see blood or a small amount of fluid at the injection site, simply wipe the site with the alcohol wipe and apply light pressure.
Medication Administration • Intramuscular (big needle) injection • Clean the injection site with an alcohol wipe by rubbing in a circular motion. Remove the needle cap. • Stretch the injection site with one hand and using the other hand, quickly insert the needle straight in as far as it will go. • Release the skin. With that hand draw back very gently on plunger; if no blood flows into the syringe, inject the medication. If blood is seen, the needle is probably in a vein - remove the needle and apply pressure to the needle site. Repeat the injection at another site after putting on a new needle. • Remove the needle. Rub the area in a circular motion to massage the medication. Dispose of the syringe in a “sharps” container. If you see blood or a small amount of fluid at the injection site, simply wipe the site with the alcohol wipe and apply light pressure.
Monitoring Instructions • U/S and Blood work • Vaginal probe U/S to check size and number of follicles (fluid sacs in the ovary containing the eggs) • Male and female U/S technicians • Blood test for estradiol and/or progesterone
Monitoring Instructions • Where/when • Weekdays • 7-8a in U/S L-1 for U/S and bloods • 7-9a 3rd floor for bloods only • Weekends • 7:30-8:30a in U/S L-1 for U/S and bloods
Monitoring Instructions • Standing order lab slip • Do not write on it • Filed in lab for 1 year • Tell lab tech what test you need • Ultrasound slips • Given to you in ultrasound
Monitoring Instructions • Fill out a call back sheet each time you test • Name and phone numbers • Voice messages: Yes or No • Have identifiers on your answering machines • Leave room on the answering machine for the longest incoming message available
Monitoring Instructions • Satellite testing centers • 850 Boylston (weekdays only) • Use BWH testing slips (see Instruction booklet for times) • Patriot’s Place, Foxboro (weekdays only) • Use BWH testing slips (see Instruction booklet for times)
Daily Cycle Instructions • Daily orders are done by the doctors by 2p • Nurses call with new instructions by 5p • If there is no call by 5p, page the F&E Fellow on call 617-732-6660
Pre-Operative Appointment • During the stimulation • Meet with MD and anesthesiologist to sign surgical consents • On a testing day if BWH patient • If testing at a satellite, test at BWH on the day of the pre-op appointment
Day of Egg Retrieval (ER) • Admission to 5C • No eating/drinking after midnight the night before • Bring hospital blue card • Arrive 5C 1 hr before ER • Admit to pre-op/recovery area • Change into a hospital gown • IV started • Couple together pre/post op
Day of Egg Retrieval • Operating room • Feet in stirrups • Anesthesia • U/S guidance, needle inserted into each follicle, fluid removed by suction • Fluid passed to embryologists who remove eggs from the fluid • By stretcher to the recovery room
Sperm collection • In advance • If you need to be together or produce at home notify your nurse • If you anticipate a problem with production, consider freezing specimens before the cycle starts • Day of HCG shot • Ejaculation within 5 days before the egg retrieval • Abstain after HCG shot
Sperm collection • Day of Egg Retrieval • Bring hospital blue card and a picture ID • Produce specimen • Day of egg retrieval • Private room on 5C • Fill out paperwork and label specimen container • No lubricants
Day of Egg Retrieval • Post op recovery • 1 - 1 1/2 hours • Need a ride home • May feel groggy, sore, backache • Pain medication prescription • Start antibiotics; also medrol if ICSI, PGD, AH
Day after Egg Retrieval • Post op recovery • Fertilization call • Start progesterone (if Crinone start tomorrow); also Estrace if ICSI, PGD, AH • Take it easy for 48 hours
Day of Embryo Transfer (ET) • You will get a call the afternoon before the ET with the transfer time • Arrive 1 hour before transfer time • Do not empty your bladder
Day of Embryo Transfer • MD will discuss the embryos with you • Couple can be together for the ET • 10 minutes to recover • Take it easy for 24 hours
Cancellation • Poor response to medication • Few or no follicles; low estradiol • Estrogen level and follicle number don’t match • Missed testing or medication • Ovulation before egg retrieval • No fertilization • Arrested development of embryos
Possible Complications of ARTClick on an item below to go directly to that page. Once there, hit the arrow on the page to get back here. • Multiple pregnancy • OHSS • Infection at injection or operation site • Ectopic (tubal) pregnancy • Ovarian torsion (twisting) • Medication side effects • Surgical risks
Embryo Freezing • Sign consent and NECC contract • Freeze good quality embryos • Notification if you have frozen embryos • Cryo embryo transfer cycle (CET) • Insurance company may require it Liquid Nitrogen embryo storage tank
Pregnancy Test • Approximately 18 days after the egg retrieval • If you have bleeding, do not stop progesterone • Cycle review after negative test or +FH
EMERGENCIES • If you have an emergency • Call 617-732-6660 • Ask for the F & E fellow on call • Stay on the line or leave a call back number and the physician will return your call
Typical IVF Cycle • Call with your period • Suppression therapy 7-21 days • Baseline U/S and/or blood • Start the stimulation • 7-14 days later HCG • 36 hours later egg retrieval • 3-5 days later embryo transfer • 16 days later pregnancy test
Consents • Consent booklet • Multiple consent forms • Cannot start cycle without signed consents • Arrange to give them to your nurse
Nurse Appointment • If you need more assistance, call to make an appointment with your nurse to: • Review your individual protocol • Discuss medications and pharmacies • Learn how to do injections
Multiple pregnancy Because several follicles containing eggs can mature and ovulate at the same time, it can result in a multiple pregnancy. Thus multiple implantation of embryo can occur. Usually, the number of fetuses can be determined by ultrasound at 6-7 weeks gestation (4 -5 weeks after the IUI). Fetal reduction may be possible in high order multiple gestation pregnancies. Complications
Ovarian Hyperstimulation Syndrome (OHSS) After ovulation, the follicles fill up with fluid and form cysts. Thiscan lead to lower abdominal discomfort and bloating. Symptoms of OHSS may include: nausea and vomiting, shortness of breath, weight increase 2-3 pounds a day, low urine output. These can happen within 2 weeks after the HCG injection. The symptoms usually resolve within 1-2 weeks without treatment. Pregnancy can make it worse and last longer. Treatment may include cancelling the cycle before the HCG and in severe cases hospitalization for fluid management. Complications
Infection at the injection site Symptoms of injection site infection can include redness and/or extreme tenderness at the site and fever (rare). You may be instructed to apply warm soaks to the site and/or be given antibiotic treatment. Ectopic pregnancy (tubal pregnancy) You will have an early ultrasound to rule out ectopic pregnancy. Approximately 5% of Assisted Reproduction pregnancies become ectopic and resolve on their own or are treated with medication or surgery. Symptoms may include abdominal pain and/or irregular bleeding. Complications
Ovarian torsion (twisting) In less than 1% of cases, the enlarged ovary can twist on itself. This can decrease the blood supply to the ovary and result in significant lower abdominal pain. Surgery may be required to untwist or possibly remove the ovary. Medication side effects Read the package inserts of your medications and discuss any possible side effects with your physician. Complications
Surgical risks Infection: Bacteria may be transferred into the abdominal cavity by the retrieval needle. Bleeding: The retrieval needle goes through the vaginal wall and into the ovary. These have blood vessels and there are other blood vessels nearby. Trauma: It is possible to damage nearby abdominal or pelvic organs. Anesthesia: Complications such as: allergic reaction, low blood pressure, nausea or vomiting. Failure: The egg retrieval could fail to get any eggs or the eggs may be abnormal or of poor quality and may not fertilize or produce a viable pregnancy. Complications