Download
1 / 57
580 likes | 671 Views
Explore the intricate anatomy of the hip joint, its ligaments, and arthrokinematics. Learn how to assess hip conditions and perform detailed examinations to diagnose issues. Discover red flags and clinical presentations related to hip, pelvis, and thigh problems.

E N D
Anatomy • Ball & Socket joint • Convex femoral head: 2/3 covered with cartilage • Head of femur points in anterior, medial, superior direction
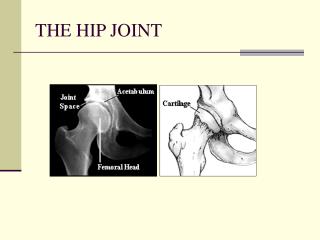
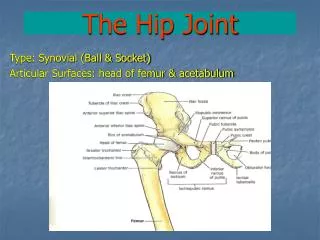
Anatomy • Acetabulum faces lateral, inferior and anterior direction • Ring of cartilage covers periphery • Labrum • Triangular fibrocartilaginous ring attached to the bony rim of the acetabulum • Serves to deepen the socket & increase surface area; thereby increasing stability • Improves mobility by providing an elastic alternative to a bony rim
Anatomy • Collum (neck) of Femur • 3-5 cm long • 115-128 degree angle of inclination • 10-15 degree angle with the frontal plane axis of the femoral condyles (anteversion)
How do we check the anteversion angle? Craig’s Test – • patient prone knee flexed 90o • Palpate posterior aspect of greater trochanter. • Passive internal rotation the hip > greater trochanter in its most lateral position. • If the angle is > 15 degrees in IR, the femur is considered to be in anteversion.
Anatomy • Pulvinar acetabuli, fat pad located in the acetabular fossa • Lubrication • Shock absorber • Protects ligamentum teres
Anatomy • Joint capsule shaped like a cylindrical sleeve – 4 sets of fibers: • Longitudinal • Oblique • Arcuate • Circular • Deep fibers of rectus femoris strengthen capsule anteriorly
Anatomy • Ligaments • Ligamentum Teres • Iliofemoral ligament • Pubofemoral ligament • Ischiofemoral ligament
Arthrokinematics & ROM • Flexion/Extension:120°/20° • Spin movement of the head of the femur • Adbuction: 45° • Head of the femur glides inferior • Adduction: 30° • Head of the femur glides superior • Internal Rotation: 30° • Head of the femur glides posterior • External Rotation: 45° • Head of the femur glides anterior
Clinical Presentation • Resting position • 30° flexion, 30° abduction, 20° ER • Close packed position • Extension, abduction, internal rotation • Capsular pattern • Flexion, abduction, IR • Sometimes IR is most limited. Order may vary, but will always include these 3 movements
Hip Examination • Medical Screening • Outcome Measure • Subjective Examination • Objective Examination • Intervention • HEP Hypothesis?
Red Flags for Hip, Pelvis & Thigh • Colon CA • Pathologic Fractures of Femoral Neck • Avascular Necrosis • Legg-Calve-Perthes Disease • Slipped Capital Femoral Epiphysis
Colon CA History Exam Finding Later Stages – hypo- or hyperactive bowel sounds TTP abdomen in area of CA Possible Ascites First sign may be mets to: liver, lung, brain • >50yoa • bowel disturbances • unexplained weight loss • Hx colon CA in immediate family • pain unchanged by change in position
Pathologic Fracture of Femoral Neck History Exam Findings Severe constant pain, worse with movement Shortened LE LE in ER position • Older women >70yoa with hip, groin, or thigh pain • Hx fall from a standing position
Osteonecrosis History Exam Findings Gradual onset of pain worse with weight bearing Stiff hip joint – most limited with IR & flexion • Long term corticosteroid use • Osteonecrosis in the contralateral hip • Traume
Legg-Calve-Perthes History Exam Findings Antalgic gait Aggravated with movement – hip abduction & IR • 5-8yo males • Presenting with hip/groin pain
Slipped Capital Femoral Epiphysis History Exam Findings Aching in groin increased by weight bearing LE held in ER Limited IR of hip • Overweight Adolescent • Hx of recent growth spurt or trauma
Hip Examination • Medical Screening • Outcome Measure • Subjective Examination • Objective Examination • Intervention • HEP Hypothesis?
Hip Specific Historical Examination • Questions: • Do your symptoms change (better or worse) with any movements of the low back? Do you have any pain in your low back, even if you feel it is unrelated to your hip pain? • Does your hip pain extend down into your thigh or leg? Do you ever experience numbness or tingling into the hip, thigh, leg ankle or foot? • Have you recently increased your physical activity, especially running (distance, terrain, speed) or other weight bearing activities? • Do you have pain or stiffness in the hip or groin region? Do you have a family history of osteoarthritis? Morning stiffness <60 minutes? Pain with prolonged walking? • Do you experience clicking, catching, or giving way of the hip? Do your symptoms worsen with full flexion or extension? Ref: Flynn TW, Cleland JA, Whitman JM. Users’ Guide to the Musculoskeletal Examination. Evidence in Motion. ISBN 978-0-9714792-3-4.
Hypothesis? Physical Examination serves to support/refute your working hypothesis/hypotheses
Seated Examination • Neuro exam if indicated • Myotomes • Dermatomes • MSR • Note alteration in areas of peripheral nerve sensation • ROM • Hip IR/ER • MMT (as indicated) • Hip flexors • Hip IR/ER • Knee extensors • Ankle dorsiflexors
Standing Examination • Lumbar • A/P/OP ROM • Observation • Standing: observe anterior, posterior and lateral for asymmetry of: • Soft tissues or bony landmarks of hip, gluteal region, low back, lower extremities • Gait: abnormal gait mechanics and/or reproduction of symptoms • Palpation • Iliac crest • ASIS • PSIS • Greater trochanter • Special Tests (as indicated) • Standing flexion (SIJ)
Supine Examination • ROM (A/P/OP) • Flexion • IR/ER • Abduction • Flexibility • HS • Piriformis (>90/<90° flexion) • Iliopsoas, RF, ITB (Thomas test) • Observation/Palpation • Iliac crest, ASIS • Malleoli (after leveling) • Inguinal ligament • Joint Mobility • Anterior glide • Posterior glide • Inferior glide • Long axis distraction • Special Tests (as indicated) • Scour • FABER • SLR • Sign of the buttock • Leg length • Compression/Distraction (SIJ) • Supine to sit (SIJ)
Side-lying Examination • Flexibility • ITB (Ober’s Test) • MMT • Hip Abductors
Prone Examination • Palpation • Iliac crest/PSIS • Sacral sulcus • ILA • Ischial tuberosity • ROM (A/P/OP) • Hip extension • Flexibility • Rectus Femoris (Ely’s test) • Joint Mobility • Anterior glide • Posterior glide • MMT • Hip extensors • Knee flexors • Special Tests (as indicated) • Flick test (SIJ) • Deerfield (SIJ)
DIFFERENTIAL DIAGNOSIS What is common?
Hip Osteoarthritis • Moderate to severe OA affects more than 22 million American adults between ages 24-74 yrs (Mikesky et al 2006) • Incidence study showed rates of 0.5/1000 per year of people with hip OA (Felson et al, 1987)
Loss of hyaline cartilage Sub-chondral bone sclerosis Joint space loss Osteophyte formation Pathology of Hip Osteoarthritis
Diagnosis • Many patients often have symptoms of hip and knee OA early in its course without radiographic changes and 40% of patients with typical radiographic changes may be asymptomatic. Therefore, subject matter experts recommend the diagnosis of hip & knee OA not be based on radiographs alone (Altman et, 1986; Balint et al, 1996)
Test Item Cluster for Hip Osteoarthritis • Test Cluster 1: • Self reported squatting as an aggravating factor • Passive hip IR ROM <25° • Active hip flexion causing lateral hip pain • Active hip extension increases pain • Scour’s + for pain Diagnostic Accuracy: • If 4/5 components of the test cluster are present: + LR=24.3 This increases the probability of having hip OA to 91% Ref: Sutlive et al. JOSPT 2008
PT for Hip OA – Hoeksma 2004 • RCT, n = 109, 29 week follow-up • 9 treatments • Manual PT + Exercise vs Exercise alone • Clinically meaningful improvements (pain, ROM, function) at 6 mos • Manual therapy treatment: Long axis manipulation + stretching
Manual Therapy and Exercise Group • Traction of hip joint • Traction • Traction manipulations • Stretch: • Quadriceps • Tensor fascia lata • Adductors • Sartorius • Gracilis
Stretches Exercises to increase motion Muscle strengthening exercises Balance activities Home exercise program Exercise Group
Results of the Harris Hip Score Results on range of joint motion from flexion to extension
Both strengthening and aerobic exercise can reduce pain and improve function. 2. Prescription of exercise is essential core aspect of management of hip OA 3. Exercise should be individualized 4. Exercise adherence is important 5. Effectiveness of exercise is independent of radiographic severity
Let’s back up the truck… • Where is all this OA coming from? • Possibility of undiagnosed and untreated underlying movement dysfunctions, FAI, or hip labral tears?
FAI Abnormal abutment between the acetabulum and femoral head causing progressive cartilage erosion: “Cam” – femoral head “Pincer” – acetabular
Clinical Findings with FAI Macfarlane RJ, Haddad FS. The diagnosis and management of femoro-acetabular impingement. Ann R Coll Surg Engl 2010; 92:363–367. • Flexion and IR painful that is intermittent with repeated hip activities • May c/o: • Clicking • Snapping • Popping • Radiographic findings of the bony anomaly
FAI • Precursor for labral tears (responsible for large proportion) and hip OA • Predisposers for FAI: • Genetic morphological anatomy • Slipped femoral epiphysis • Legg-Calve-Perthes • Hip dysplasias • Malunited fractures
Surgical Intervention for FAI • Early recognition with possible surgical repair to avoid the degenerative changes in the hip and labral damage • Philippon et al in a prospective analysis of 112 patients undergoing primary hip arthroscopy for symptomatic FAI, demonstrateda significant improvement in pre-operative Harris hip scores (HHS) from a mean of 58 to a postoperative mean of 84, at a mean follow-up of 2.3 years.
Labral Tears Groh MM, Herrera J. A comprehensive review of hip labral tears. Curr Rev Musculoskelet Med 2009; 2:105–117 [13, 30]. • Labral Function: • Stability • Shock absorption • Pressure distribution (increases the surface area by 28%) and lubrication • Etiology of Labral Tears: • Trauma • femoroacetabular impingement (FAI) • capsular laxity/hip hypermobility • Dysplasia • Degeneration
Labral Tears • Clinical Presentation: • anterior hip or groin pain • frequently with mechanical symptoms: • Clicking • Locking • Giving way
Diagnosis of Labral Tears Frequently undiagnosed for an extended period of time… • Initially will perform plain radiographs to assess for dysplasia, degeneration, and other causes of pain. • Magnetic resonance arthrography (MRA) is the diagnostic test of choice, with arthroscopy being the gold standard. • Magnetic resonance imaging (MRI) and computed tomography scans are unreliable for diagnosis.
Soft Tissue Injuries • Trochanteric bursitis: • Bursa becomes irritated and inflamed due to excessive compression and repeated friction as ITB snaps over bursa • Psoas bursitis: • Pain in groin or anterior thigh, maybe into patellar area • Aggravated with activities requiring excessive hip flexion • Ischiogluteal bursitis: (Tailor’s/Weaver’s Bottom) • Pain @ ischial tuberosities especially when sitting
Gluteus medius Piriformis Superior Gemellus Obturator internus Inferior Gemellus Quadratus femoris