Download
1 / 31
330 likes | 566 Views
Chapter 21. The Nutrition Care Process. Nutrition Care Process. Assess nutritional status. Analyze data to identify nutritional needs. Plan and prioritize nutritional care objectives to meet these needs. Implement strategies necessary to meet the objectives.

E N D
Chapter 21 The Nutrition Care Process
Nutrition Care Process • Assess nutritional status. • Analyze data to identify nutritional needs. • Plan and prioritize nutritional care objectives to meet these needs. • Implement strategies necessary to meet the objectives. • Evaluate the nutritional care outcomes.
Patient/Nutrition Care Process • Admission • MD orders: PE, Dx, PMHx, Diet order, Labs, Tests/Procedures, Consults, Meds RN Assessment: Ht, Wt, I/Os, Vitals, PO, FPG, Allergies, GI Status, Feeding ability/Dentition, Wounds • Nutrition Screen: Age, Dx, Diet Rx, Anthros, Labs, Oral intake, GI, Meds
Nutriton AssessmentGather & evaluate/analyze data Update screen info from MR Interview pt/family D/w staffDocument assessment & plan SOAP, PIE, DAR, Narrative Paper vs. computer chart
Implement Strategies (Interventions) • Education, Referrals, Food Preferences, snacks/supplements • Nutrition F/U Assessments • Evaluate outcomes, Document assessment, • Implement further strategies PRN
Nutritional Assessment • The process by which the nutritional status of an individual is determined • Usually includes dietary history and intake data, laboratory data, clinical examination and health history, anthropometric data, and psychosocial data
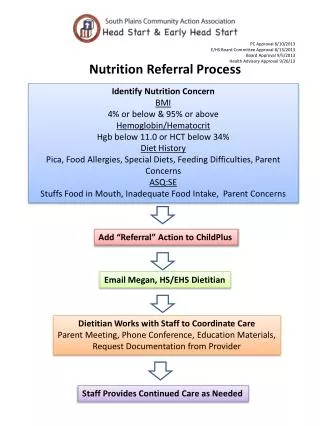
Nutrition Screening and Assessment Tool Courtesy Carolinas Medical Center, Charlotte, N.C.
Development of a Plan for Nutritional Care • Prioritize problems • Client and counselor must jointly establish achievable goals • Express objectives in behavioral terms • State objectives in quantifiable terms
Implementation of Nutritional Care • Implementation is the component of the nutritional care process that translates assessment data into strategies, activities, or interventions that will enable the patient or client to meet the established objectives. • Interventions should be specific: —What? —When? —Where? —How?
Evaluation of Nutritional Care • Evaluate care provided • Review plan frequently • Reassess plan—may be new needs • Identify any new needs • Formulate a new nutritional care plan
Nutritional Care Record • Written documentation of the nutritional care process, including the interventions and activities used to meet the nutritional objectives
Care Record Courtesy St. John’s Hospital, Springfield, Ill.
Documentation Style • DAP (diagnosis, assessment, plan) • PIE (problem, intervention, evaluation) • PES (problem, etiology, symptoms) • IER (intervention, evaluation, revision) • HOAP (history, observation, assessment, plan) • SAP (screen, assess, plan) • SOAPIER (subjective, objective, analysis/assessment, plan, intervention, evaluation, revisions) • SOAP (subjective, objective, assessment, plan)
SOAP Notes S: Subjective • Info provided by patient, family, or other • Pertinent socioeconomic, cultural info • Level of physical activity • Significant nutritional history
SOAP Notes—cont’d O: Objective • Factual, reproducible observations • Diagnosis • Height, age, weight—and weight gain patterns • Lab data • Clinical data (nausea, diarrhea) • Diet order • Medications
SOAP Notes—cont’d A: Assessment • Interpretation of patient’s status based on subjective and objective info • Evaluation of nutritional history • Assessment of laboratory data and medications • Assessment of diet order • Assessment of patient’s comprehension and motivation
SOAP Notes—cont’d P: Plan • Diagnostic studies needed • Further workup, data needed • Medical nutrition therapy goals • Recommendations for nutritional care
Nutritional Care of the Terminally Ill Patient • Maintenance of comfort and quality of life are the main goals of nutritional care for terminally ill patients. • Dietary restrictions are rarely appropriate.
Palliative Care • Encourages the alleviation of physical symptoms, anxiety, and fear while attempting to maintain the patient’s ability to function independently
Discharge Planning Discharge documentation includes • Summary of nutritional therapies and outcomes • Pertinent information such as weight, lab results, dietary intake • Potential drug-nutrient interactions • Expected progress or prognosis • Recommendations for follow-up services
Discharge Planning Courtesy University of Washington Medical Centers, Seattle.