Download
1 / 70
780 likes | 1.2k Views
The Nutrition Care Process: Driving Effective Intervention and Outcomes. Nutrition Care Process. Process for identifying, planning for, and meeting nutritional needs Malnutrition increases: morbidity length of hospital stay = more care mortality higher costs ($$$$$$$). Ø.

E N D
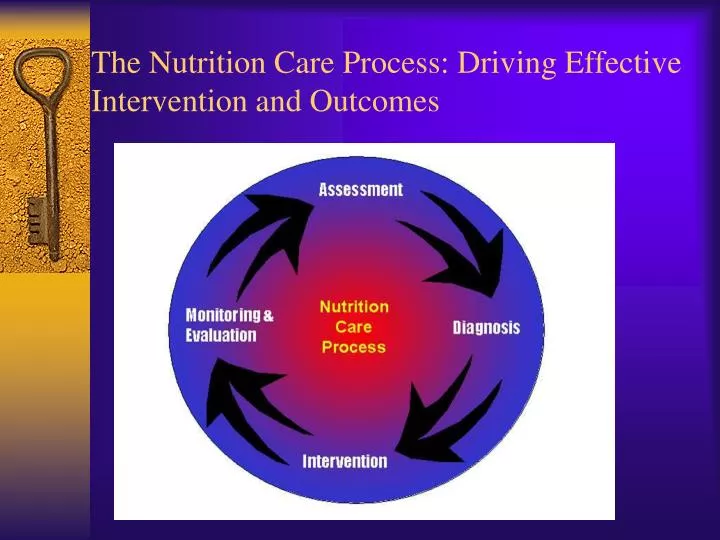
The Nutrition Care Process: Driving Effective Intervention and Outcomes
Nutrition Care Process • Process for identifying, planning for, and meeting nutritional needs • Malnutrition increases: • morbidity • length of hospital stay = more care • mortality • higher costs ($$$$$$$)
Ø ADA NUTRITION CARE PROCESS AND MODEL Screening & Referral System Ø Identify risk factors Ø Use appropriate tools and methods Ø Involve interdisciplinary collaboration Nutrition Diagnosis Ø Identify and label problem Nutrition Assessment Ø Determine cause/contributing risk Ø Obtain/collect timely and factors appropriate data Ø Cluster signs and symptoms/ Ø Analyze/interpret with defining characteristics evidence - based standards Ø Document Document Relationship Between Patient/Client/Group Nutrition Intervention Dietetics & Ø Plan nutrition intervention · Professional Formulate goals and determine a plan of action Implement the nutrition intervention Ø · Care is delivered and actions Nutrition Monitoring and - are carried out Evaluation Ø Documen t Ø Monitor progress Ø Measure outcome indicators Ø Evaluate outcomes Ø Document Outcomes Management Sys tem Ø Monitor the success of the Nutrition Care Process implementation Ø Evaluate the impact with aggregate data Ø Identify and analyze causes of less than optimal performance and outcomes Ø Refine the use of the Nutrition Care Process
Central Core of Nutrition Care Model The relationship between the client & the dietetics professional(s) • collaborative • client-focused • individualized
Outer Rings of Nutrition Care Model • Strengths brought to process by dietetics professional • dietetics knowledge • skills of critical thinking, collaboration, communication • evidence-based practice • Factors of external environment • health care system, practice setting • social support, economics, education level
ADA’s Nutrition Care Process Steps • Nutrition Assessment • Nutrition Diagnosis • Nutrition Intervention • Nutrition Monitoring and Evaluation For more information, access the ADA member page in the Quality Management section. http://www.eatright.org/Member/83_12962.cfm
Nutrition Assessment Components • Gather data, considering • Dietary intake • Nutrition related consequences of health and disease condition • Psycho-social, functional, and behavioral factors • Knowledge, readiness, and potential for change • Compare to relevant standards • Identify possible problem areas
Example of Nutrition Assessment Content • Type of assessment • Content component • Nutritional adequacy • Fat and cholesterol intake • Trans fatty acid intake • Health status • Lipid profile • BMI • Waist circumference • What are the reliable • standards (ideal goals)? • how well, how much, • how long Nutrition assessment what data are most effective for identifying clients’ nutrition related problem of interest What type of assessment data?
How do we get from Assessment to Intervention?Nutrition Diagnosis A crucial element of providing quality nutrition care
Nutrition Diagnosis Purpose • Identify and label the nutrition problem • Nutrition diagnosis NOT medical diagnosis • EXPLICIT statement of nutrition diagnosis Note: Documentation is an on-going process that supports all the steps in the Nutrition Care Process
Nutrition Intervention Purpose • Plan and implement purposeful actions to address the identified nutrition problem • bring about change • set goals and expected outcomes • client-driven • based on scientific principles and best available evidence Note: Documentation is an on-going process that supports all the steps in the Nutrition Care Process
Nutrition Monitoring & Evaluation Purpose • Determine the progress that is being made toward the client’s goals or desired outcomes Monitoring: review and measurement of status at scheduled times • Evaluation: systematic comparison with previous status, intervention goals, reference standard Note: Documentation is an on-going process that supports all the steps in the Nutrition Care Process
Nutrition Screening Purpose: To quickly identify individuals who are malnourished or at nutritional risk and to determine if a more detailed assessment is warranted Usually completed by DTR, nurse, physician, or other qualified health care professional At-risk patients referred to RD
Characteristics of Nutrition Screening Simple and easy to complete Routine data Cost effective Effective in identifying nutritional problems Reliable and valid
Nutrition Screening Tools Acute-care hospital or residential setting Perinatal service Pediatric practice Malnutrition Universal Screening Tool (MUST) Nutrition Screening Initiative (NSI)
Food and Nutrient Intake Risk Factors • Calorie or protein, vitamin and mineral intake greater or less than required • Swallowing difficulties • Gastrointestinal disturbances, bowel irregularity • Impaired cognitive function or depression • Unusual food habits (pica) • Misuse of supplements • Restricted diet • Inability or unwillingness to consume food • Increase or decrease in activities of daily living Hammond KA. Assessment: Dietary and Clinical Data. In Krause, 12th edition, p. 386
Psychological/Social Risk Factors • Language barriers • Low literacy • Cultural or religious factors • Emotional disturbances associated with feeding difficulties (e.g., depression) • Limited resources for food preparation or obtaining food or supplies • Alcohol or drug addiction • Limited or low income • Lack of ability to communicate needs • Limited use or understanding of community resources Hammond KA. Assessment: Dietary and Clinical Data. In Krause, 12th edition, p. 386
Physical Risk Factors • Extreme age (adults >80 years, premature infants, very young children) • Pregnancy: adolescent, closely spaced, or three or more pregnancies • Alterations in anthropometric measurements, marked overweight/ underweight for age, height, both; depressed somatic fat and muscle stores • NOTE: recent unintentional weight loss is more predictive of morbidity/mortality than wt/ht status Hammond KA. Assessment: Dietary and Clinical Data. In Krause, 12th edition, p. 386
Physical Risk Factors (cont) • Chronic renal/cardiac disease, diabetes, pressure ulcers, cancer, AIDS, GI complications, hypermetabolic stress, immobility, osteoporosis, neurological impairments, visual impairments Hammond KA. Assessment: Dietary and Clinical Data. In Krause, 12th edition, p. 386
Abnormal Laboratory Values • Visceral proteins (albumin, prealbumin, transferrin) • Lipid profile (cholesterol, HDL, LDL, triglycerides) • Hemoglobin, hematocrit, other blood tests • BUN, creatinine, electrolytes • Fasting and PP blood glucose levels, A1C Hammond KA. Assessment: Dietary and Clinical Data. In Krause, 12th edition, p. 386
Medications • Chronic use • Multiple and concurrent use (polypharmacy) • Drug-nutrient interactions
Joint Commission Standards Drive Nutrition Screening in Health Care Organizations
Nutrition Care Process: Screening • The Joint Commission (TJC) requires that nutritional risk be identified within 24 hrs in all hospitalized pts • TJC also requires nutrition screening in accredited ambulatory facilities • Standards of Care protocols determines process; evidence-based guidelines • Use simple techniques, available info • May be done by other than RD • Usually simple form with targeted info
Standard PC.2.20:The hospital defines in writing the data and information gathered during assessment and reassessment Elements of Performance • The information...to be gathered during the initial assessment includes the following, as relevant...: • Each patient's nutrition and hydration status, as appropriate • The hospital has defined criteria for when nutritional plans must be developed
Standard PC.2.120: The hospital defines in writing the time frame(s) for conducting the initial assessment(s). Elements of Performance • A nutritional screening, when warranted by the patient's needs or condition, is completed within no more than 24 hours of inpatient admission • CAMH online version, 2006
Standards Relating to Nutrition Assessment Standard PC.2.130 • Initial assessments are performed as defined by the hospital. Standard PC.2.150 • Patients are reassessed5 as needed.CAMH online version, 2006
Screening for Malnutrition in Acute Care Settings “The consensus of the committee is that while screening for nutrition risk in the acute care setting is crucial, the JCAHO requirement that nutrition screening be completed within 24 hours of admission is not evidence-based and may produce inaccurate and misleading results.” • Institute of Medicine, 1999
Diagnosis Weight Weight change Need for diet modification or education Laboratory values (s. albumin, cholesterol, hemoglobin, TLC Problems with chewing or swallowing Diarrhea Constipation Food dislikes or intolerance Commonly Used Criteria for Nutrition Risk Screening-Acute Care Institute of Medicine, 1999
Nutrition Screening and Assessment Tool Courtesy Carolinas Medical Center, Charlotte, N.C.
Prevalence of Nutrition Risk in Acute Care • The prevalence of nutrition risk will vary depending on the population screened and the criteria used for screening • In published studies, prevalence of malnutrition in hospitalized patients has ranged from 12% to more than 50% • There is little published data regarding nutrition screening for other purposes
CNM Nutrition Screening SurveyChima and Seher, 2007 • Blast email sent to 1668 members of the Clinical Nutrition Management dietetic practice group in May, 2007 • 522 usable surveys were returned, for a response rate of 31%
Does Your Health Care Organization Screen Patients for Nutrition Risk? (with accredited ambulatory clinics)
Who Has Primary Responsibility for Nutrition Screening (Inpatient)? % of Respondents *In the 1987 survey, only 60% of 77 respondents reported admission nutrition screening
If Nursing Screens, Do Nutrition Staff Do a Secondary Screen?
Criteria Used by Nutrition Staff in Secondary Screening (n=258)
Criteria Used by Nutrition Staff in Secondary Screening (n=258)
Where Is Secondary Screening Documented in the Medical Record?
Criteria Used by Nursing/Nutrition to Identify Patients at Nutrition Risk (Inpatient)
Criteria Used By Nursing/Nutrition to Identify Patients at Nutrition Risk (Inpatient)