Download
1 / 1
10 likes | 137 Views
RIPPLE Pathway: Realising Individual Patient Preferences at Life's End. The patient’s condition is deteriorating and death could occur in the next few hours, days or weeks. Reversible causes have been considered by the team

E N D
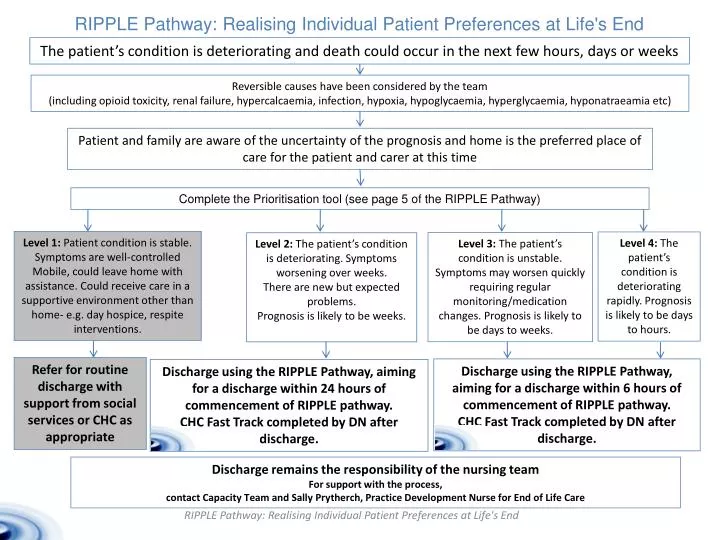
RIPPLE Pathway: Realising Individual Patient Preferences at Life's End The patient’s condition is deteriorating and death could occur in the next few hours, days or weeks Reversible causes have been considered by the team (including opioid toxicity, renal failure, hypercalcaemia, infection, hypoxia, hypoglycaemia, hyperglycaemia, hyponatraeamia etc) Patient and family are aware of the uncertainty of the prognosis and home is the preferred place of care for the patient and carer at this time Complete the Prioritisation tool (see page 5 of the RIPPLE Pathway) Level 1: Patient condition is stable. Symptoms are well-controlled Mobile, could leave home with assistance. Could receive care in a supportive environment other than home- e.g. day hospice, respite interventions. Level 4: The patient’s condition is deteriorating rapidly. Prognosis is likely to be days to hours. Level 3: The patient’s condition is unstable. Symptoms may worsen quickly requiring regular monitoring/medication changes. Prognosis is likely to be days to weeks. Level 2: The patient’s condition is deteriorating. Symptoms worsening over weeks. There are new but expected problems. Prognosis is likely to be weeks. Refer for routine discharge with support from social services or CHC as appropriate Discharge using the RIPPLE Pathway, aiming for a discharge within 6 hours of commencement of RIPPLE pathway. CHC Fast Track completed by DN after discharge. Discharge using the RIPPLE Pathway, aiming for a discharge within 24 hours of commencement of RIPPLE pathway. CHC Fast Track completed by DN after discharge. Discharge remains the responsibility of the nursing team For support with the process, contact Capacity Team and Sally Prytherch, Practice Development Nurse for End of Life Care RIPPLE Pathway: Realising Individual Patient Preferences at Life's End