Download
1 / 28
470 likes | 1.48k Views
Bronchiectasis. Chapter 14 – Des Jardins P. 584-589 – Merck Manual. Objectives. State the clinical definition for Bronchieactasis Describe the anatomic alterations of the lungs in Bronchieactasis Describe the etiology of Bronchieactasis

E N D
Bronchiectasis Chapter 14 – Des Jardins P. 584-589 – Merck Manual
Objectives • State the clinical definition for Bronchieactasis • Describe the anatomic alterations of the lungs in Bronchieactasis • Describe the etiology of Bronchieactasis • List the clinical manifestations seen in Bronchieactasis. Include findings of the physical examination, laboratory tests, pulmonary function tests, chest x-rays, arterial blood-gas values, and hemodynamic indices. • Describe the management of Bronchieactasis.
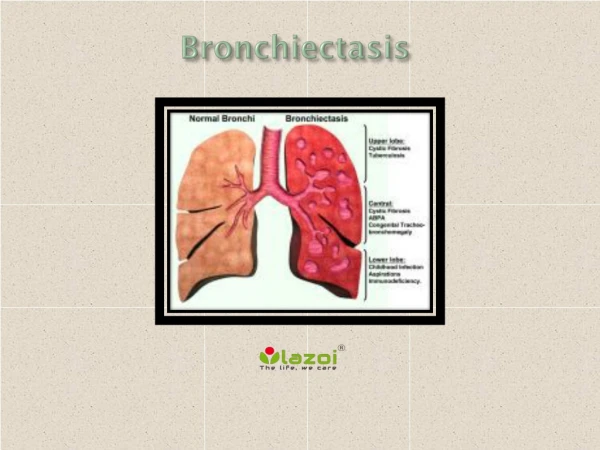
Definition • A chronic dilation and distortion of one or more bronchi due to extensive inflammation and destruction of the bronchial wall cartilage, blood vessels, elastic tissue and smooth muscle.
Etiology • Usually occurs secondary to: • Repeated, severe pneumonia • Measles, Pertussis, Adenovirus in children • Klebsiella • Staphylococci • Influenza virus • Fungal infections • Myocbacteria • Mycoplasma • Bronchial Obstruction • Congenital Defect • Manifestation of Cystic Fibrosis • Kartagener’s Syndrome • Primary ciliary dyskinesia (PCD)
Etiology (cont.) • Idiopathic • Accounts for roughly 50 to 80% of cases • Possible immunologic defect or autoimmune abnormality. • Immune-related diseases • Allergic bronchopulmonary aspergillosis (ABPA) • Collagen Vascular diseases • Rheumatoid arthritis • Sjögren syndrome • Ulcerative colitis • Crohn’s disease • Immune deficiencies (?)
Pathophysiology • Either one or both lungs may be involved. • It is commonly limited to a lobe or segment and is frequently found in the lower lobes. • Right Middle Lobe and Left Lingula also possible. • Extent and character of pathologic changes determines the functional abnormalities. • Increased mucus production with impaired mucociliary clearance • Changes in lung volumes distal to obstruction • Increased due to Ball-Valve effect • Decreased due to atelectasis • Reduced flow rates • / defects with hypoxemia
Types of Bronchiectasis Varicose Saccular Technically there are 2 other kinds: Follicular and Traction. But….who cares? Cylindrical
Varicose Bronchiectasis • Bronchi are dilated and constricted in an irregular fashion similar to varicose veins. • Varicose bronchiectasis is also called fusiform.
Cylindrical Bronchiectasis • Bronchi are dilated and have regular outlines similar to a tube. The dilated bronchi fail to taper for 6-10 generations and then in the bronchogram appear to end squarely because of mucous obstruction
Saccular Bronchiectasis • Bronchi progressively increase in diameter until they end in large, cyst-like sacs in the lung parenchyma. • This form causes the greatest damage to the tracheobronchial tree. • The bronchial walls become composed of fibrous tissue. • Cartilage, elastic tissue and smooth muscle are all absent.
Anatomic Alterations • Copious amounts of bronchial secretions. • Mucociliary clearance mechanism is impaired. • Foul smelling mucous from anaerobic organisms. • Mucous plugs cause partial or complete obstruction. • Hyperinflation of the distal alveoli as a result of an expiratory check valve obstruction. • Atelectasis, consolidation, and fibrosis results from complete bronchial obstruction.
Pathophysiology • Obstructive Lung Diseases but can have a restrictive component if alveolar lung volumes are reduced. • Obstructive and Restrictive Disease
Physical Examination • Vital Signs: • f: Increased (tachypnea). • HR: Increased • BP: Increased (Increased CO) • Inspection: • Pursed lip breathing. • Cyanosis. • Prolonged expiratory phase. • Increased A-P diameter • Digital clubbing
Physical Examination • Palpation: • Use of accessory muscles during I & E. • Percussion: • Hyperresonant if obstructive, Dull if restrictive. • Auscultation: • Inspiratory crackles and/or rhonchi. • May be diminished if obstructive, bronchial with restrictive.
Physical Assessment • Chief complaint: • Cough with large volume of sputum • Hemoptysis • Sputum settles into distinct layers with streaks of blood often seen • Thick, tenacious sputum • Chronic sinusitis is a common complaint. • Also nasal polyps • Kartagener’s Syndrome (Bronchiectasis, dextrocardia & paranasal sinusitis). • 20% of Bronchieactasis is as a result of Kartagener’s.
ABG • Mild to Moderate Bronchiectasis • Acute alveolar hyperventilation with hypoxemia. • Severe Bronchiectasis • Chronic ventilatory failure with hypoxemia. • Oxygenation Indices • Increased shunting. • Decreased oxygen delivery.
Pulmonary Function Studies • Obstructive Disease • Decreased FVC and FEV1.0 • Decreased Flowrates • Increased RV, FRC, TLC, RV/TLC • Restrictive Defect • Reduced RV, FRC, TLC • RV/TLC ratio normal • Flows are normal.
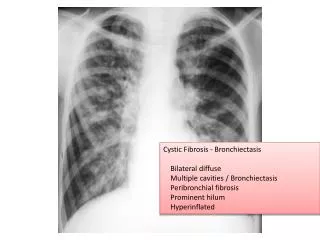
Chest X-ray • Obstructive Lung Disease • Translucent (dark) lung fields • Depressed, flattened diaphragms • Long, narrow hearts • Right ventricular enlargement • Restrictive Process • Atelectasis and consolidation • Increased opacity
Laboratory Findings • Culture and Sensitivity • Haemophilus influenzae • Streptococcus pneumoniae • Staphylococcus aureus • Pseudomonas aeruginosa • Anaerobic organisms • Sputum separates into layers • CBC • Polycythemia and increased WBC (infection).
Diagnosis • Bronchography (Bronchogram) • Injection of opaque contrast material into the TB tree • Rarely done. • High-Resolution CT Scan • Bronchial walls appear thick, dilated. • Replaced standard CT scan and Bronchography as gold standard.
Prophylaxis • Awareness and early identification may allow for earlier intervention. • Childhood immunizations. • Reduce exacerbations.
Treatment Goals • Reduce infections/exacerbations • Manage secretions • Reduce airway obstruction • Treat complications • Hemoptysis • Hypoxemia • Respiratory Failure • Cor Pulmonale
Treatment • Antibiotics to treat pneumonia • Inhaled steroids to reduce inflammation • Oxygen therapy (low FiO2) • Bronchial Hygiene Protocol • CPT/PD • Hydration • Deep breathing/coughing • Humidification
Therapy • Aerosol Therapy • Mucolytics • Bronchodilators • Flu shots/Pneumonia Vaccinations • Bronchoscopy • Avoidance of respiratory irritants • Surgical resection • Saccular is most suitable for surgery
Prognosis • Mild Bronchiectasis – may have a normal life span • Extensive Bronchiectasis – shorter life span • Result of respiratory infection and complications • Disease of slow deterioration interspersed by episodes of exacerbation