Download
1 / 26
320 likes | 1.24k Views
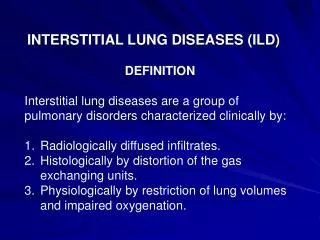
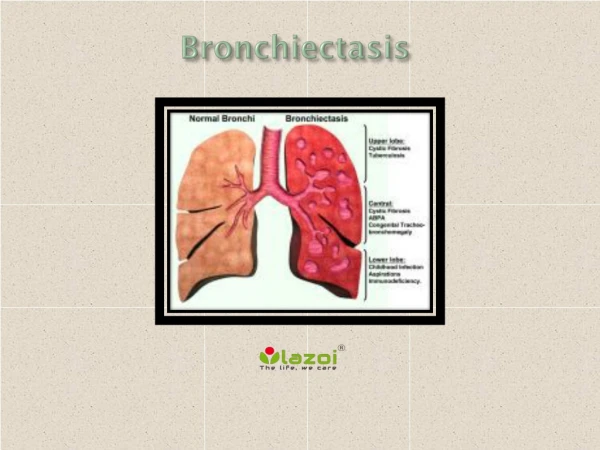
Bronchiectasis & Suppurative Lung Diseases. By Dr. Abdelaty Shawky Assistant professor of pathology. 1. Bronchiectasis. 2. Lung abscess. 3. Empyema. 1. Bronchiectasis. * Def: persistent dilatation of medium sized bronchi accompanied by suppurative inflammation of their walls.

E N D
Bronchiectasis& Suppurative Lung Diseases By Dr. Abdelaty Shawky Assistant professor of pathology
1. Bronchiectasis. 2. Lung abscess. 3. Empyema.
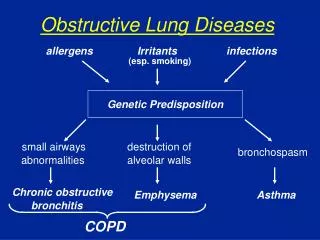
* Def:persistent dilatation of medium sized bronchi accompanied by suppurative inflammation of their walls. * Etio-pathogenesis: I. Weakening of the bronchial wall by; a. Chronic suppurative inflammation: due to recurrent septic bronchopneumonia. b. Congenital weakness: leads to congenital bronchiectasis. II. Bronchial obstruction: by foreign body, bronchial secretion or tumor.
* N/E: - Dilated bronchi: • Cylindrical, fusiform or saccular • Bilateral. • Basal. • Has patchy distribution. • The bronchial lumen contains pus. • The bronchial mucosa: ulceratd. - The surrounding alveoli are: fibrotic and collapsed. - The pleura shows: pleurisy - Draining hilar L. nodes:enlarged
* Complications: • Spread of infection: direct, lymphatic and blood. • Hemoptysis. • Lung abscess (post-bronchiectatic lung abscess). • 2ry amyloidosis. • Lung fibrosis. • Bronchogenic carcinoma (squamous cell carcinoma).
* Definition:A localized suppurativeinflammmation due to pyogenic bacteria. * Types: 1. inhalation (aspiration) lung abscess. 2. Pyaemic lung abscesses. 3. post-pneumonic lung abscess. 4. lung abscess complicating other conditions.
I. Inhalation (aspiration) lung abscess * Etiology: • Inhalation or aspiration of septic material from upper respiratory tract, or vomitus in persons under general anesthesia or in coma. * Morphology: • The Rt. lung is commonly affected. • Single, related to a peripheral bronchus. • Two forms; acute abscess & chronic abscess.
* Complications: • Spread of infection: Direct, lymphatic & blood. • Rupture leads to hemoptysis and bronchopleural fistula. • Lung gangrene (due to putrifaction by saprophytic bacteria. • Lung fibrosis leads to pulmonary hypertension. • 2ry Amyloidosis: in chronic lung abscess.
II. Pyaemic lung abscesses • Are multiple abscesses due to pulmonary pyaemiai.e arrest of septic emboli in the pulmonary vasculature. * Morphologically: • Multiple. • Affect both lungs, usually peripheral (subpleural). • Related to small blood vessels. • Uniform in size & shape.
III. Post-pneumonic lung abscess • Single or multiple abscesses complicating pneumonia.
IV. Lung abscess complicating other conditions • Follow Bronchiestasis. • Secondary infected bronchogenic carcinoma. • Infected hydatid cyst. • Spread from subdiaphragmatic abscess. • Penetrating chest injury.
* Clinical Course: • The manifestations of pulmonary abscesses are much like those of bronchiectasis and are characterized principally by cough, fever, and copious amounts of foul-smelling purulent or sanguineous sputum.
Diagnosis of this condition can be only suspected from the clinical findings and must be confirmed by chest X.ray. • Whenever an abscess is discovered, it is important to rule out an underlying carcinoma because this is present in 10% to 15% of cases.
The course of abscesses is variable. With antimicrobial therapy, most resolve with no major sequelae.
* Definition: accumulation of purulent pleural exudate in the pleural space due to bacterial seeding. * Source of infection: • Most commonly, this seeding occurs by contiguous spread of organisms from intrapulmonary infection, but occasionally, it occurs through lymphatic or hematogenous dissemination from a more distant source.
Rarely, infections below the diaphragm, such as the subdiaphragmatic or liver abscess, may extend by continuity through the diaphragm into the pleural spaces, more often on the right side.
* Morphology: Empyema is characterized by loculated, yellow-green, creamy pus composed of masses of neutrophils admixed with other leukocytes. Although empyema may accumulate in large volumes (up to 500 to 1000 mL), usually the volume is small, and the pus becomes localized.
* Course: • Empyema may resolve, but this outcome is less common than organization of the exudate, with the formation of dense, tough fibrous adhesions that frequently obliterate the pleural space or envelop the lungs; either can seriously embarrass pulmonary expansion.