Download
1 / 37
450 likes | 880 Views
Fontan Circulation. Nick Collins July 12 2011. Why?. Congenital Heart Disease Too much is never enough Champagne EP Echo for the discerning Beyond EF…. High end structural interventions Haematology Respiratory medicine Phil Roberts Context Jeff Pretto ASD Fenestrations….

E N D
Fontan Circulation Nick Collins July 12 2011
Why? • Congenital Heart Disease • Too much is never enough • Champagne EP • Echo for the discerning • Beyond EF…. • High end structural interventions • Haematology • Respiratory medicine • Phil Roberts • Context • Jeff Pretto • ASD • Fenestrations….
Unfamiliar • Outline • Questions • Not too many slides…. • Garry…. • Fontan in principle • Rationale • Late issues • Management • Imaging • Cross sectional
If Nothing Else…. • Palliative operation for functionally single/uni ventricular heart • Not perfect repair • 70% survival at 25 years • Prone to late complications • Case to illustrate
Fontan • Single ventricle • Underlying congenital heart disease varies • Typically hypoplastic right ventricle • Morphologic LV supporting circulation • HLHS • End result of two/three operations • Initial description tricuspid atresia • Others • No subpulmonary ventricle • Creates a circulation in series, rather than parallel • Passive blood flow into pulmonary circulation • Illustrate
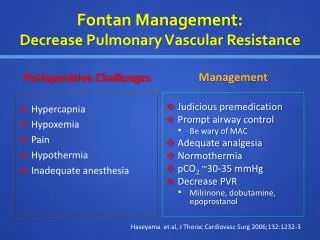
Passive Filling • Requires elevated venous pressure • Certain requirements • Requires pressure gradient for filling (ie cannot rely on RV systolic function) • Low systemic ventricle EDP • No AV valve regurgitation • No outflow tract obstruction • Low PA pressure/PVR • Fenestration • Any condition affecting PVR • Chest infection • PE • Sleep disordered breathing
Pulmonary Vascular Bed • Low flow • Not pulsatile • Thrombogenic • Need for aspirin/warfarin • Contraception • Pregnancy
Passive Filling • Requires elevated venous pressure • Certain limitations • Hypovolaemia • Diuretic therapy • Elevated JVP is essential! • Laparoscopic surgery • Diminished venous return
Early Iterations • Dilated right atrium • Prone to atrialarrythmia • Universal problem • Warfarin • More physiological versions • Bypass the right heart • Two methods • Lateral tunnel • Incorporates right atrial tissue • Extra cardiac
ASD vs Fenestration • Single ventricle • Functionally single atria • Surgically created ASD • Fenestration • Communication between atria and Fontan circuit • Concern regarding PVR • Cyanosis vs venous congestion • Concern regarding systolic function • Prevent elevated EDP
Any Problems….. • Universal to ACHD • Highlight specific • Arrhythmia • 50% after 20 years • Poorly tolerated – ventricular dysfunction • Atrial tachycardia • IART • AF/atrial flutter • Medical therapy • Young… • Ablation • Expand…. • Fontan conversion • Early iterations • Lateral tunnel/extra-cardiac • Arrhythmia surgery
Arrhythmia • Bradycardia • Medication side effects • Implications “newer” generations • Unable to access atrial tissue • Unable to position leads into right/subpulmonary ventricle • Epicardial systems • Anticoagulation
Other Late Problems… • Introduce case • 17 year old male • Previously followed CHW • “Adult” • Functional single ventricle • Double inlet left ventricle • TGA • VSD • Pulmonary stenosis
Blalock Taussig shunt • Glenn shunts (Bilateral SVC) • Aim to preserve pulmonary blood flow • Fontan completion age 4 • Since well • No therapy • Asymptomatic
Baseline Assessment • ECG • Torment registrars • Echocardiography • Exercise stress test • Pathology • Hb 185-200 • Normal albumin
Echocardiography and the Fontan • Difficult • Ability to identify • IVC/SVC • Phasic flow • Outflow tract • Anastamosis PA and Aorta (DKS) • Pulmonary vessels • Critical – cross sectional imaging • Serial assessment • EF • Tissue Doppler • Dp/Dt • No reference ranges/nomograms
Summarise • Stable effort tolerance • Reduced compared to peers • Hypoxaemia at rest/exercise • Secondary erythrocytosis
Exercise capacity in adults with CHD- Impact of underlying diagnosis Mean ± SD Aortic coarction 28.7 ± 10.4 Tetralogy of Fallot 25.5 ± 9.1 VSD 23.4 ± 8.9 Mustard-operation 23.3 ± 7.4 Valvular disease 22.7 ± 7.6 Ebsteins anomaly 20.8 ± 4.2 Pulmonary atresia 20.1 ± 6.5 Fontan-operation 19.8 ± 5.8 ASD (late closure) 19.2 ± 6.2 ccTGA 18.6 ± 6.9 Complex anatomy 14.6 ± 4.7 Eisenmenger 11.5 ± 3.6 ANOVA p<0.0001 5 10 15 20 25 30 35 40 Peak VO2 (ml/kg/min) Diller GP, et al.Circulation 2005; 112:828-35.
Late Complications • Hypoxaemia • Residual fenestration • Importance operation report • TOE/Cath/MRI • Collateral formation • Porto-systemic collaterals • High filling pressures • Pulmonary AV fistulae • Initial Fontan • Classic Glenn shunt • RA to right PA anastamosis
All Downhill…. • Left sided pleuritic chest pain • No previous episodes • No infective symptoms • No cough/haemoptysis • Unchanged effort capacity • Unchanged ECG
Fontan and PE • Varma et al JACC 2003 Jun 18; 41(12):2252-8 • TCCCA • 17% PE on V/Q – CTPA • None on warfarin • Potentially critical in “attrition” • Increased pulmonary resistance
Fontan and PE • Warfarin • Protective in context atrial arrhythmia • Predisposes to anaemia • Warfarin/Fontan/Renal impairment • Patients with univentricular/systemic right ventricles • Difficult to evaluate • Elevated baseline Hb
Additional Late Complications • Arrhythmia • Ventricular dysfunction • Multiple contributing mechanisms • Strong association with: • Symptoms • Clinical heart failure in 40% Fontan • Piran et al Circulation 2002: 105:1189-1194 • Objective exercise capacity • Arrhythmia risk • Mortality • Protein Losing Enteropathy (PLE)
PLE • Most problematic • Progressive hypoproteinaemia • Aetiology unclear • Possible venous congestion • Incidence 1-15% • High mortality rate • No successful treatment options • Medical • Surgical • Transplant • Higher mortality compared to other CHD
Back to business….. • Progressively fatigued • Difficulty in attending University • Headache • Role of increased Hb • Underwent venesection • Transient improvement • Cyanosis/effort tolerance • Cardiac Catheter
Closure right to left shunt • Fenestration alone • Amplatzer type device • More diffuse • Covered stent • Booked August….
Summarise • Fontan • Final common surgical pathway for single ventricle physiology • Imperfect repair • Life long follow up • Life expectancy • Transplant • Late complications • Arrhythmia • Ventricular dysfunction