Download
1 / 19
240 likes | 528 Views
The clinical manifestations of abcess and focal infections due to local spread, hematogenous d/s associated with immune deficiency and how they differ from the mimics. Brain Abscess.

E N D
The clinical manifestations of abcess and focal infections due to local spread, hematogenous d/s associated with immune deficiency and how they differ from the mimics
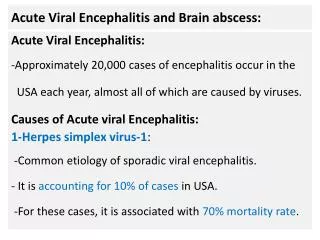
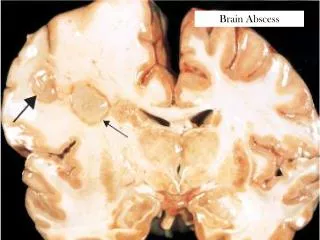
Brain Abscess • A brain abscess is a collection of immune cells, pus, and other material in the brain, usually from a bacterial or fungal infection. • Majority is always secondary to purulent focus elsewhere in the body (only 10% introduced from the outside) • 40% related to d/s in the paranasal sinuses, middle ear and mastoid cells • Purulent pulmonary infection
Brain Abscess • Mortality/Morbidity • With the introduction of antimicrobics and imaging 5-15% decrease in Mortality Rate. • Rupture of a brain abscess, however, is associated with a high mortality rate (up to 80%). • The frequency of neurological sequelae in persons who survive the infection varies from 20-79%. • Sex • More common in males. • Age • Brain abscesses occur more frequently in the first 4 decades of life.
Pathophysiology • Caused by intracranial inflammation with subsequent abscess formation. • In at least 15% of cases, the source of the infection is unknown (cryptogenic). • Infection may enter the intracranial compartment directly or indirectly via 3 routes. • Three Routes: • Contiguous suppurative focus • Hematogenous spread from a distant focus • Trauma
Contiguous suppurative focus Bone of the middle ear or nasal sinuses becomes the seat of osteomyelitis Spread along the veins Abcess at a considerable distance from primary site of focus
Hematogenous spread from a distant focus • 1/3 of all brain abcess • Majority -ABE and septic focus on the lungs or pleura • Others - congenital heart defect, pulmonary AV malformation • Middle cerebral artery • multiple
Trauma • 10% of cases • Open skull fracture allows organisms to seed directly in the brain. • Brain abscess can also occur as a complication of intracranial surgery, foreign body, bullets, and shrapnel.
Clinical Diagnosis • The symptoms and signs include the following: • Low- or high-grade fever • Persistent headache (often localized) • Drowsiness • Confusion • Stupor • General or focal seizures • Nausea and vomiting • Focal motor or sensory impairments • Papilledema • Ataxia • Hemiparesis
Clinical Diagnosis • The symptoms and signs include the following: • Localized neurologic signs • Cerebellar abscess - Nystagmus, ataxia, vomiting, and dysmetria • Brainstem abscess - Facial weakness, headache, fever, vomiting, dysphagia, and hemiparesis • Frontal abscess - Headache, inattention, drowsiness, mental status deterioration, motor speech disorder, hemiparesis with unilateral motor signs, and grand mal seizures. • Temporal lobe abscess - Headache, ipsilateral aphasia (if in the dominant hemisphere), and visual defect.
Causes • Anaerobic and microaerophiliccocci and gram-negative and gram-positive anaerobic bacilli are the most important isolates. • The predominant organisms include the following: • Staphylococcus Aureus • Aerobic, anaerobic, and microaerophilic streptococci, including alpha-hemolytic streptococci and Streptococcus milleri • Bacteriodes, Prevotella, and Fusobacterium species • Enterobacteriaceaeorganisms, including Klebsiella pneumonia, Escherichia coli, and Proteus species (Rare isolates include Enterobacter species, Actinobacillusactinomycetemcomitans, and Salmonella species) • Pseudomonas species • Other anaerobes
Differential Diagnosis • Cryptococcosis • Cysticercosis • Epidural Abscess • Meningitis
Laboratory Studies • Routine tests • CBC count with differential and platelet count • Erythrocyte sedimentation rate (ESR; elevated in up to two thirds of patients) • Serum C-reactive protein (CRP) or Westergren sedimentation rate • Serological tests for some pathogens (eg, serum immunoglobulin G antibodies, CSF polymerase chain reaction for Toxoplasma) • Blood cultures (at least 2; preferably before antibiotic usage) • Results: • Moderate leukocytosis is present, • ESR and CRP level are generally elevated. • Serum sodium levels may be low because of inappropriate antidiuretic hormone production. • Platelet counts may be high or low.
Laboratory Studies • Cerebrospinal fluid • Elevated protein level, pleocytosis with variable neutrophil count, a normal glucose level, and sterile cultures. • A lumbar puncture is mostly of value to rule out other disease processes, especially bacterial meningitis. • The white blood cell reaches 100,000/µL or higher when the abscess ruptures into the CSF. • Many red blood cells are generally observed at that time, and the CSF lactic acid level is then elevated to more than 500 mg. • Abscess aspirate (obtained via stereotactic CT or surgery) • Culture aspirates of abscesses for aerobic, anaerobic, and acid-fast organisms and fungi • Gram stain, acid-fast stain (for Mycobacterium), modified acid-fast stain (for Nocardia), and special fungal stains (eg, methenamine silver, mucicarmine) • Histopathological examination of the brain tissue.
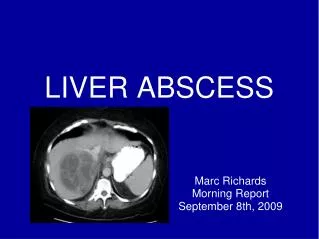
Imaging Studies • CT imaging of the brain (with and without contrast) is the most readily available study for establishing diagnosis of brain abscess • Early in the course: abscess appears as a low-density, irregular zone • As the disease progresses: distinctive "ring enhancement“
Other Causes of Pus • subdural empyema (from sinusitis, mastoiditis - rare, 20% mortality) • meningitis, encephalitis, AIDS, toxoplasmosis (see Neurology Chapter) • osteomyelitis of skull (Pott’s puffy tumour), usually seen with sinusitis • granuloma (TB, sarcoid)
Surgical Measures • mandatory when neurologic deficits are severe or progressive • used when the abscess is in the posterior fossa • Abscess drainage - (via needle) under stereotactic CT guidance through a burr hole under local anesthesia, is most rapid and effective method. May be repeated if needed. • Craniotomy - if abscess is large or multilocular
Treatment • Antibiotics according to organism if known • Pen G and metronidazole, or chloramphenicol if unknown • Add oxacillin or nafcillin if trauma or IV drug user ; use vancomycin in penicillin-sensitive patients • If gram(-)organism suspected (otic, GI, GU organ) add third-generation cephalosporin • Abscess associated with HIV infection assumed to be due to Toxoplasma gondii - daily doses of sulfadiazine and pyrimethamine.
Treatment • Anticonvulsants - phenytoin until abscess resolved or perhaps longer. Obtain anticonvulsant levels. • Following surgical procedure - corticosteroids to reduce edema. Dexamethasone. Taper rapidly. Use usually limited to 1 week. Continue antibiotics for 6-8 weeks.