Download
1 / 25
320 likes | 706 Views
Brain abscess. Brain abscess (or cerebral abscess) is an abscess caused by inflammation and collection of infected material within the brain tissue., coming from

E N D
Brain abscess (or cerebral abscess) is an abscess caused by inflammation and collection of infected material within the brain tissue., coming from • local (ear infection, dental abscess, infection of paranasal sinuses, infection of the mastoid air cells of the temporal bone, epidural abscess) • or remote (lung, heart, kidney etc.) infectious sources,
The infection may also be introduced through a skull fracture following a head trauma or surgical procedures. • Brain abscess is usually associated with congenital heart disease in young children. It may occur at any age but is most frequent in the 3rd third decade of life. • Deadly brain abscesses due to infection caused from tongue piercing have occurred
Features • The symptoms of brain abscess are caused by a combination of • increased intracranial pressure due to a space-occupying lesion (headache, vomiting, confusion, coma), • infection (fever, fatigue etc.) and • focal neurologic brain tissue damage (hemiparesis, aphasia etc.). • The most frequent presenting symptoms are • headache, drowsiness, confusion, seizures, hemiparesis or speech difficulties together with fever with a rapidly progressive course.
Features • The symptoms and findings depend largely on the specific location of the abscess in the brain. • An abscess in the cerebellum, for instance, may cause additional complaints as a result of brain stem compression and hydrocephalus. • Neurological examination may reveal a stiff neck in occasional cases (erroneously suggesting meningitis). • The famous triad of fever, headache and focal neurologic findings are highly suggestive of brain abscess.
Many brain abscesses are polymicrobical. The predominant organisms include: • Staphylococcus aureus, • aerobic and anaerobic streptococci (especially Streptococcus intermedius), • Bacteroides, Prevotella, and Fusobacterium species, Enterobacteriaceae, Pseudomonas species, and other anaerobes. • Less common organisms include: Haemophillus influenzae, Streptococcus pneumoniae and Neisseria meningitides.[
Bacterial abscesses rarely (if ever) arise de novo within the brain, although establishing a cause can be difficult in many cases. • There is almost always a primary lesion elsewhere in the body that must be sought assiduously, because failure to treat the primary lesion will result in relapse.
location of the primary lesion • for example in compound skullfractures where fragments of bone are pushed into the substance of the brain, the cause of the abscess is obvious. Similarly, bullets and other foreign bodies may become sources of infection if left in place. • The location of the primary lesion may be suggested by the location of the abscess: • infections of the middle ear result in lesions in the middle and posterior cranial fossae; • congenital heart disease with right-to-left shunts often result in abscesses in the distribution of the middle cerebral artery; • and infection of the frontal and ethmoid sinuses usually results in collection in the subdural sinuses.
predisposing conditions: • Sinus and dental infections— streptococci, anaerobic GNR (e.g. Prevotella, Porphyromonas, Bacteroides), Fusobacterium, S. aureus, and Enterobacteriaceae • Penetrating trauma—S. aureus, aerobic streptococci, Enterobacteriaceae, and Clostridium spp. • Pulmonary infections— streptococci, anaerobic GNR (e.g. Prevotella, Porphyromonas, Bacteroides), Fusobacterium, Actinomyces, and Nocardia • Congenital heart disease—Aerobic and microaerophilic streptococci, and S. aureus • HIV infection—T. gondii, Mycobacterium, Nocardia, Cryptococcus, and Listeria monocytogenes • Transplantation—Aspergillus, Candida, Cryptococcus, Mucorales, Nocardia, and T. gondii • Neutropenia—Aerobic GNR, Aspergillus, Candida, and Mucorales
Protozoa • Toxoplasma gondii • Entamoeba histolytica, • Trypanosoma cruzi, • Schistosoma, • Paragonimus, & • Helminths • Taenia solium
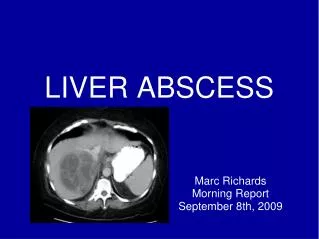
DIAGNOSIS • The diagnosis is established by a computed tomography (CT) (with contrast) examination. • At the initial phase of the inflammation (which is referred to as cerebritis), the immature lesion does not have a capsule and it may be difficult to distinguish it from other space-occupying lesions or infarcts of the brain. • Within 4–5 days the inflammation & dead brain tissue are surrounded with a capsule, which gives the lesion the famous ring-enhancing lesion appearance on CT examination with contrast (since intravenously applied contrast material can not pass through the capsule, it is collected around the lesion and looks as a ring surrounding the relatively dark lesion).
DIAGNOSIS • Ring enhancement may also be observed in cerebral hemorrhages and some brain tumors. • However, in the presence of the • rapidly progressive course with • fever, • focal neurologic findings (hemiparesis, aphasia) & • signs of increased intracranial pressure, the most likely diagnosis should be the brain abscess.
Lumbar puncture • procedure, which is performed in many infectious disorders of the central nervous system is contraindicated in this condition (as it is in all space-occupying lesions of the brain) because removing a certain portion of the CSF may alter the ICP balances and causes the brain tissue to move across structures within the skull (brain herniation)
Treatment • The treatment includes • lowering the increased intracranial pressure & • starting intravenous antibiotics (and meanwhile identifying the causative organism mainly by blood culture studies)
Treatment • Surgical drainage of the abscess remains part of the standard management of bacterial brain abscesses. • The location and treatment of the primary lesion also crucial, as is the removal of any foreign material (bone, dirt, bullets, and so forth).
For Surgical drainage here are few exceptions • Haemophilus influenzae meningitis is often associated with subdural effusions that are mistaken for subdural empyemas. These effusions resolve with antibiotics and require no surgical treatment. • Tuberculosis can produce brain abscesses that look identical to conventional bacterial abscesses on CT imaging. Surgical drainage or aspiration is often necessary to identifyMycobacterium tuberculosis, but once the diagnosis is made no further surgical intervention is necessary.
Prognosis • It was once fatal before the CT era, now, • if the abscess is treated before the person goes into a coma, then the death rate has been estimated from 5% to 20% • although it is greater in cases of multiple abscesses, when raised intracranial pressure is observed and depending on the level of neurological dysfunction on presentation. • Early treatment and the patients overall health has an effect on prognosis. • Other factors include: • antibiotic resistance or • the abscess location. An abscess deep within the brain is more difficult to treat than others.
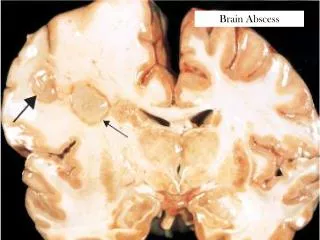
a)represent the abscess contents, the middle zone (b) formed by proliferating fibroblasts resembling a fibrocollageous capsule & outermost one (c) formed by gliotic and inflammed brain parenchyma
S. anginosus group is commonly isolated from brain abscesses