Download
1 / 54
720 likes | 1.45k Views
Preoperative Assessment. Professor Lester AH Critchley. Purpose of anaesthetist’s visit. Assessment of patient for anaesthesia Discuss the anaesthetic with patient Planning anaesthetic management Prepare patient for anaesthesia. Assessment of patient. General fitness of patient

E N D
Preoperative Assessment Professor Lester AH Critchley Med 5: Anaeshesia
Purpose of anaesthetist’s visit • Assessment of patient for anaesthesia • Discuss the anaesthetic with patient • Planning anaesthetic management • Prepare patient for anaesthesia Med 5: Anaeshesia
Assessment of patient • General fitness of patient • Specific problems: • Medical • Technical • Anaesthetic drug • Psychological Med 5: Anaeshesia
General fitness of patient • Most important: • Cardio-respiratory reserve • How & why? • Context of the surgical procedure Med 5: Anaeshesia
Medical problems • Disease processes • Medical therapies Med 5: Anaeshesia
Disease processes • COAD • Heart disease • Hypertension • Heart failure • Valvular heart disease • Diabetes • Others: • Liver failure • Kidney failure • Thyroid Med 5: Anaeshesia
ASA classification:American Society of Anesthesiologists physical status Additional categories added since June 2005 ASA 5 A moribund patient who is not expected to survive without the operation ASA 6 A declared brain-dead patient whose organs are being removed for donor purposes Med 5: Anaeshesia
A 27-year old business man admitted for removal of nasal polyps. He has allergic rhinitis and bronchial asthma, for which he takes regular beconase (steroid) and ventolin inhalers. • A 75-year old man admitted for a transurethral resection (TURP) following an episode of acute retention of urine, due to benign prostatic hypertrophy (BPH). He has severe chronic bronchitis and is limited to walking only 100 yards on the flat before he has to stop to regain his breath. He has had numerous hospital admissions for his chest. • A 35-year old secretary with past good health admitted for an emergency laparoscopic appendectomy. She has a two day history of abdominal pain. • A middle-aged insulin dependant diabetic admitted for an eye operation proceedure. The patient is known to have significant renal dysfunction with high creatinine levels and she is CAPD. • A 92-year old demented woman is admitted with a ruptured aortic aneurysm. She is hypotensive and struggling to breathe. • A 45-year old school teacher admitted for a total abdominal hysterectomy for uterine fibroids. She is a type 2 diabetic controlled by oral hypoglycaemic drugs and diet. She has been a diabetic for several years and has no major complications from her disease. Med 5: Anaeshesia
Ongoing treatments Antihypertensives Anticonvulsants Routes of admission Oral vs IV Anticoagulants Warfarin Heparin Aspirin & NSAIDs (Regional blocks) Steroids Pituitary-adrenal suppression Psychiatric Antidressants MAO inhibitors Lithium Medical therapies Med 5: Anaeshesia
Technical problems • *Airway (& assessment) • *IV access (&assessment – inspection) • Spinal access • Others • Cervical spine injury • Deformities • Obesity • Neonates Med 5: Anaeshesia
Outline of upper airway TONGUE Posterior tongue & epiglottis obstruct view of larynx. During laryngoscopy they are displaced forward by scope blade Med 5: Anaeshesia
The LEMON guide:Physical signs for predicting difficult intubation? • Look externally, • Evaluate the 3-3-2 rule, • Mallampati, • Obstruction, • Neck mobility Med 5: Anaeshesia National Emergency Airway Management Course
Look externally Med 5: Anaeshesia
Evaluate the 3-3-2 rule Med 5: Anaeshesia
Mallampati classification Med 5: Anaeshesia
Mallampati score? Med 5: Anaeshesia
Anaesthetic Drugs • Allergies & Anaphyllaxis • Inherited disorders • Scoline apnoea • Malignant hyperpyrexia • Porphyria Med 5: Anaeshesia
Allergies & Anaphyllaxis • Althesin story • Older muscle relaxants, i.e. Alcuronium • Lignocaine & the airway • Newer & cleaner drugs today Med 5: Anaeshesia
Inherited disorders • Succinylcholine apnoea • Plasma cholinesterase enzyme • Prolonged paralysis • Malignant hyperpyrexia • Defect of calcium in the muscle cells • Triggers – halothane / succinylcholine • Rigidity, high CO2, fever, death • Porphyria • Variety of syndomes including paralysis • Trigger – barbituates Med 5: Anaeshesia
Psychological problems • Children • Dementia • Mentally retarded • Downs / Cerebral palsy / Syndromes (FLKs) • Anxiety • VIP-patients Med 5: Anaeshesia
Planning anaesthetic management • Surgical procedure • Different operations different requirements • Patient factors • Anaesthetic preferences Med 5: Anaeshesia
Preparation of patient • Medically • Mentally • Prevent aspiration • Organize theatre Med 5: Anaeshesia
Medical preparation • Done mainly on the surgical ward • Covered in second lecture Med 5: Anaeshesia
Mental preparation • Explain - procedures • Discuss – choices of technique • Counsel - fears • Consent • Research Med 5: Anaeshesia
Explain“What is going happen to the me!” • Before • GA vs. Regional technique • Monitoring lines sited • Fibre optic intubation • After • Intensive care • Pain management (APS) Med 5: Anaeshesia
Discuss • Type of anaesthetic • General • Spinal / Epidural • Regional block • Type of pain relief • i.m. morphine • PCA • Regional infusion Med 5: Anaeshesia
Counsel - Fears • Death (relative died under anaesthesia) • Memory loss • Awareness • Neurological deficit (Epidural) Med 5: Anaeshesia
Neurological complications • Chesterfield Royal Hospital in 1947 • Albert Woolley (aged 56-years) and Cecil Roe (aged 45-years) were healthy, middle-aged men who became paraplegic after spinal anaesthesia for minor surgery. • The spinal anaesthetic was given by the same anaesthetist, using the same drug (cinchocaine) on the same day. The outcome for the patients and their families was devastating. • At the trail 6-years later the judge accepted the suggestion that phenol, in which the ampoules of local anaesthetic had been kept, had contaminated the local anaesthetic solution via a crack. Med 5: Anaeshesia
Consent – Anaesthetic • Dental damage • Neurological damage • Brain injury / death • Minor complications: • Pain / nausea / malaise / headache / sore throat / muscle pains Med 5: Anaeshesia
Research • New drugs • New procedures • New devices /monitors • Need consent Med 5: Anaeshesia
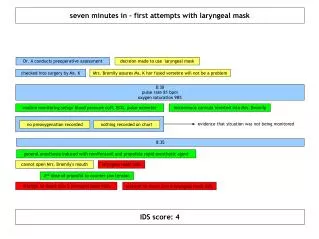
Prevent Aspiration • Why is aspiration a problem? • Preoperative fasting regimens • Antacid prophyllaxis • Rapid sequence induction • Cricoid pressure Med 5: Anaeshesia
Downward pressure is applied to the cricoid which is transferred to the oesophagus Oesophagus is closed off Med 5: Anaeshesia
Demonstration of Cricoid Pressure on a model Med 5: Anaeshesia
Rapid sequence induction • Protection against aspiration: • Insufficient preop fasting • Gastric stasis • Hiatus hernia / reflux • Pregnancy Med 5: Anaeshesia
Type Few episodes Prolonged Cause Surgery Medical condition - ↑ICP, Drug induced – morphine Treatment Cause Anti-emetic agent Maxalon 10mg Nausea & vomiting Med 5: Anaeshesia
Organization of Case • Services • ICU bed • Pain service • Equipment • Fibreoptic bronchoscope • Blood warmers / cell saver • Room temperature • Help • i.e. Difficult paediatric case Med 5: Anaeshesia
Role of the Medical Officer • Prepare patient medically for anaesthesia • Arrange things for operation • X-match blood & order blood products • Consent form • Look after patient afterwards Med 5: Anaeshesia