Download
1 / 6
60 likes | 274 Views
seven minutes in – first attempts with laryngeal mask. Dr. A conducts preoperative assessment. decision made to use laryngeal mask. checked into surgery by Ms. K. Mrs. Bromily assures Ms. K her fused vertebre will not be a problem. 8:30 pulse rate 81 bpm oxygen saturation 98%.

E N D
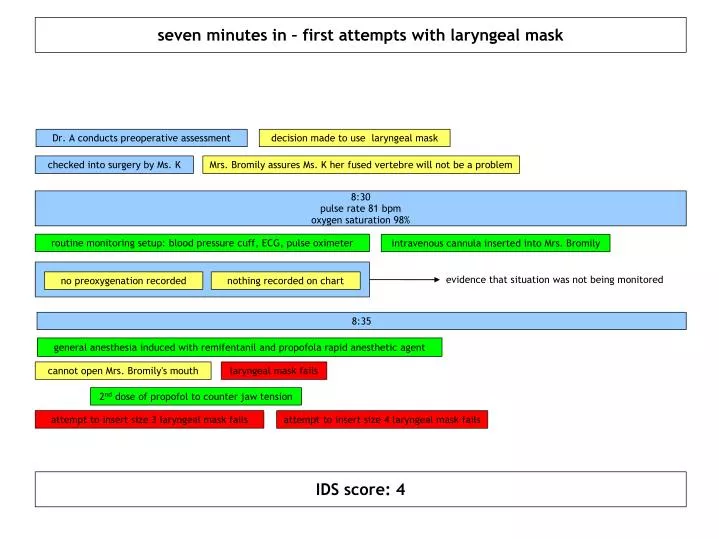
seven minutes in – first attempts with laryngeal mask Dr. A conducts preoperative assessment decision made to use laryngeal mask checked into surgery by Ms. K Mrs. Bromily assures Ms. K her fused vertebre will not be a problem 8:30 pulse rate 81 bpm oxygen saturation 98% routine monitoring setup: blood pressure cuff, ECG, pulse oximeter intravenous cannula inserted into Mrs. Bromily evidence that situation was not being monitored no preoxygenation recorded nothing recorded on chart 8:35 general anesthesia induced with remifentanil and propofola rapid anesthetic agent cannot open Mrs. Bromily's mouth laryngeal mask fails 2nd dose of propofol to counter jaw tension attempt to insert size 3 laryngeal mask fails attempt to insert size 4 laryngeal mask fails IDS score: 4
seventeen minutes in – continue ventilation / intubation attempts 8:37 Mrs. Bromily turns blue oxygenation at 75% heart rate increase 8:39 oxygen deteriorates to 40% ventilation attempt with facemask fails ventilation attempt with oral airway fails failed attempt to revise 8:41-8:43 oxygen still at bottom of chart heart rate down to 69bpm trending to 40 Dr. A attempts intubation atropine and suxamethonium administered to counter low bpm and allow intubation failed attempt to revise attempt is unsuccessful joined by Dr. B 8:45 no visual of voicebox, Carmack rating of 4; oxygen still off chart; heart rate up from atropine Mr. E and other staff enter to assist multiple attempts with full assistance failed failed attempt to revise declared can't intubate can't ventilate IDS score: 13+
twenty minutes – multiple intubation techniques 8:47-8:50 further attempts at intubation and laryngoscopy fail failed attempt to revise Dr. B attempts to use fiber optic scope and fails due to presence of blood missed opportunity to revise? may have been too late already... was Mr. E beginning his attempt already? tracheostomy set brought in 8:51-8:55 oxygen off the bottom of the chart pulse at 133bpm failed attempt to revise Mr. E attempts intubation and laryngoscopy and fails Mr. E also attempts bougie and fails 8:55 oxygen off the chart pulse at 133bpm successful insertion of laryngeal mask IDS score: 17+
fifty minutes in – post ventilation intubation attempts 9:00 oxygen up to 90% blood pressure and heart rate up steroids administered to protect from hypoxic brain damage 9:03-9:09 oxygen unstable dipping down to 49% never above 90% failed attempt to revise attempt to insert tube with fiber optic scope fails attempt to insert tube blindly fails 9:10 procedure abandoned attempting to awaken Mrs. Bromily 9:13-9:29 breathing begins; oxygen back to normal; blood pressure high; heart rate high Mrs. Bromily taken to recovery final IDS score: 19+
final hours 9:30 pulse 120 bpm; respiratory rate 20 bpm; blood pressure 84/33 mmHg; temperature 30.1 C; oxygen 95% Mrs. Bromily admitted to recovery unconscious Dr. A informs recovery staff that there were complications and Mrs. Bromily may be slow to wake Dr. A moves on to another patient missed opportunity to revise failure to recognize gravity of situation Mrs. Bromily shows signs of cerebral irritation Dr. A unavailable to help 11:00 unstable condition Mrs. Bromily taken to intensive care Mrs. Bromily never recovered
Reactions • At first glance the case seems to be an example of fixation • Digging deeper reveals multiple attempts at revision • Application of IDS to time line makes level of crisis salient • Lack of monitoring apparent from report • Report infers poor situation awareness among group • Brief time line prohibits any additional cognitive effort • cognitive workload already high • tracking and treatment of pulse, blood pressure, oxygenation • actions occur simultaneously and continuously Recommendations • When possible use awake fiber optic intubation • Improve salience of crisis scenario • Modify oximeter to display measurements below 40% • Modify oximeter display to make time below critical level salient • Incorporate better monitoring in the OR • Some form of tracking: manually on paper; via cameras and mics; verbalizations recorded and transcribed speech to text