Download
1 / 20
200 likes | 324 Views
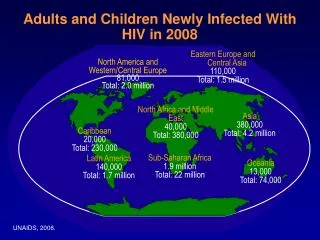
HIV-infected children born in the UK since 2000 to undiagnosed women. National Study of HIV in Pregnancy and Childhood. Pat Tookey UCL Institute of Child Health. NSHPC. HIV-infected children reported in the UK. Children born in the UK to diagnosed women

E N D
HIV-infected children born in the UK since 2000 to undiagnosed women National Study of HIV in Pregnancy and Childhood Pat Tookey UCL Institute of Child Health NSHPC
HIV-infected children reported in the UK • Children born in the UK to diagnosedwomen • Children born in the UK to women who were undiagnosed at the time of delivery • Children who were born abroad
Children with confirmed HIV infection, born to diagnosed and undiagnosed women in the UK and Ireland since 2000
Children with confirmed HIV infection, born to diagnosed and undiagnosed women in the UK and Ireland since 2000
Perinatal Transmission of HIV in England 2002-2005 Executive Summary and Recommendations available on the NSHPC and CHIVA websites www.nshpc.ucl.ac.uk/ www.chiva.org.uk/ NHS network access at nww.esussexaiau.nhs.uk/
Perinatal Transmission Audit54 children born to undiagnosed women • In a few cases antenatal testing was not offered, or having been accepted, procedures failed (delay, loss of samples or results) • At least 35% of mothers declined antenatal testing • At least 20% of children born following maternal seroconversion in pregnancy (minimum estimate) • Adverse social circumstances in many families • But based on limited information as difficult to access antenatal data • Hospital of diagnosis often not the hospital of birth • Obstetric unit often not aware of case
Summary audit recommendations… • Maximise • the current protocol to achieve even higher uptake of HIV testing in pregnancy • training, support and information for staff and women • Ensure • that all women can access the test and interventions • that all women who decline the test are offered it again, at least once by a member of the team with specialist training, preferably in 2nd trimester • that women of unknown status who arrive in late pregnancy or labour are offered rapid test as soon as appropriate
HIV prevalence1 among pregnant women by area of residence(adapted from Testing Times, HPA 2007, Fig 3.3.1) 1Unlinked anonymous survey, infant dried blood spots, Eng & Scot. Includes diagnosed and undiagnosed women.
How many women remain undiagnosed at delivery? • Probable transmission rate from undiagnosed women ~ 25% • UK prevalence estimate for pregnant women up from 0.9/1000 in 2000 to 2.3/1000 in 2006 • data only available for 360,000 births in UA survey – Scotland, London, selected English Regions • prevalence in rest of UK and Ireland probably lower • Estimated pre-delivery detection rates increased from about 75% in 2000 to 95% since 2003
How many women remain undiagnosed at delivery? • Rough estimate for 2006/7: 750,000 births a year • Overall prevalence ~2 per 1000? • 1500 infected women • If 95% are diagnosed, ~75 would remain undiagnosed at delivery • 25% transmission = ~20 infected infants per year • Consistent with reported numbers?
205 infected infants born since 2000 in the UK to undiagnosed mothers, reported to NSHPC by Sept 2008 • 51 infected infants born in 2000 to undiagnosed women reported to date • Infants born in 2001-6 • 15-30 infants reported for each year so far • Births in 2007/8 • 13 infants reported so far • Birth country / region • 40% born in London • 50% elsewhere in England • 5% in Scotland • 5% in Wales / Ireland
Country of birth (reported for 93%) 29% Zimbabwe 51% elsewhere in Africa 15% the British Isles 3% elsewhere in Europe 3% Asia or the Caribbean Age at delivery (reported for 72%) 3% under 20 years 19% 20-24 years 32% 25-29 years 35% 30-34 years 11% 35 years or older Mothers of the 205 infected children
Why were children diagnosed? • 5% following maternal screening soon after delivery • 56% following presentation with symptoms • 39% following diagnosis of another member of the family
Why were children diagnosed? • 5% following maternal screening soon after delivery • 56% following presentation with symptoms • 39% following diagnosis of another member of the family • Could some infections be postnatally acquired?
Among 14 infected children, born to undiagnosed mothers with documented negative antenatal test • 7 diagnosed before age 5 months • breast feeding duration minimal for most • 7 diagnosed at 5-24 months • all breast fed for at least 13 weeks, most much longer • Possible maternal infection after delivery • and transmission through breastfeeding
Breastfeeding common in this population • Information on breastfeeding for 80% • 80% of those breast fed • Duration reported for 75% • 1-6 weeks 27% • 7-12 weeks 22% • 13-26 weeks 27% • more than 6 months 26%
Latest outcome data – 205 children born to undiagnosed women • 2 known to have left UK/Ireland soon after birth • 21 (10%) known to have died (19 with AIDS diagnosis) • 52% under 6 months • 29% between 6 months and a year • 182 alive at last report • 45% have had one or more AIDS defining condition(s) • Mostly PCP, CMV, severe FTT, HIV encephalopathy
Latest outcome data – 74 children whose mothers were diagnosed • 8 known to have left country / lost to follow up • 2 known to have died • 64 alive at last report • 20% have had one or more AIDS defining condition(s) • HIV encephalopathy, PCP, CMV, severe FTT
What next? • Review of national antenatal screening guidelines considering further measures to • reduce number of infected women undiagnosed at delivery, • maximise antenatal test uptake, • identify seroconversions in pregnancy, and • improve the overall management of diagnosed women • Audit recommendation • When an infant / young child is diagnosed … seek permission to inform the obstetric unit that an infected infant was born to an undiagnosed woman, in order that procedures can be reviewed and revised (need appropriate obstetric and paediatric leads) • Enhance routine timely data collection for MTCT and develop protocol for review and feedback • maternal factors, timing of transmission etc
Acknowledgements • Royal College of Obstetricians & Gynaecologists • British Paediatric Surveillance Unit (Royal College of Paediatrics & Child Health) • Respondents to the NSHPC and everyone involved in reporting Funding • Health Protection Agency - NSHPC funding • Medical Research Council - CL Townsend, Training Fellowship Ethics • Multi-centre Research Ethics Committee (MREC/04/2/009) ICH team Principal Investigator: Pat Tookey Additional support: Catherine Peckham, Mario Cortina-Borja Co-ordinator: Janet Masters Researchers: Claire Townsend, Hiwot Haile-Selassie Administrative Assistants: Icina Shakes, Kate Francis Website: www.nshpc.ucl.ac.uk Email: nshpc@ich.ucl.ac.uk NSHPC