Download
1 / 16
160 likes | 309 Views
Suboptimal adherence associated with virologic failure and resistance mutations among patients on 1st line HAART in Bangalore, India. M. Ekstrand 1,2,3 , A. Shet 2,4 , S. Chandy 4 , G. Singh 4 , R. Shamsundar 4 , V. Madhavan 5 , S. Saravanan 5 , N. Kumarasamy 5

E N D
Suboptimal adherence associated with virologic failure and resistance mutations among patients on 1st line HAART in Bangalore, India M. Ekstrand1,2,3, A. Shet2,4, S. Chandy4, G. Singh4, R. Shamsundar4, V. Madhavan5, S. Saravanan5, N. Kumarasamy5 1University of California, San Francisco, United States, 2St John's Research Institute, Bangalore, India, 3University of California Berkeley, United States, 4St John's National Academy of Health Sciences, Bangalore, India 5YRGCARE, Chennai, India
Background Optimal adherence to antiretroviral regimens is closely associated with achieving and maintaining HIV viral suppression and preventing the development of drug resistant virus. Initial adherence rates in India encouraging, but recent data* from our team and from NACO suggest that adherence rates decline over time. Little known about local adherence patterns or the relationship between adherence and treatment outcome in this setting. No published data on the relationship between adherence and drug resistance in India *Bachani et al. 2010, Ekstrand et al. 2010
Objectives 1. Document local adherence patterns in Bangalore, India 2. Examine the relationship between adherence, treatment outcome and resistance associated mutations 3. Explore universal and local barriers to different patterns of non-adherence in this setting
Methods: Longitudinal 2-year cohort study, n=552 (baseline) Participants referred by MD, clinic clerk, and study screener Eligibility criteria: > 18 years old, HIV infected, on fixed dose antiretroviral medication, willing to participate in all follow-up visits. Face-to-face interviews administered in separate study offices by trained staff every 3 months for two years (ongoing) Blood drawn every 6 months, by trained staff phlebotomists. Analyzed by laboratories at Reliance Life Sciences, Mumbai and YRG CARE, Chennai. Study cleared by SJRI and UCSF IRBs and by ICMR.
Measures Demographics: gender, age, marital status, education, residence. CD4 cell counts HIV plasma Viral Load (sensitivity enables detection of an HIV RNA level to 100 copies/mL, Reliance Life Sciences, Mumbai) Viral Genotyping (YRGCARE, Chennai, in-house method certified by TAQAS Program and interpreted using Stanford HIV-1 Sequence Database. All relevant RT mutations analyzed) ART regimencurrent and past regimens, verified by prescription, pill container and chart review
Measures: Adherence Past month adherence (VAS) and >48 hour treatment interruptions combined: "Optimally adherent" : VAS score of ≥ 95 % and no tx interruptions "Sub-optimally adherent" : <95% adherence, tx interruptions, or both. Adherence barriers: Health-related: feeling too sick or too healthy, depressive sx Refill-related: ran out of meds, problems getting to pharmacy or clinic Regimen-related: medsside effects, perceives drugs as “toxic”, problems following MD’s instructions Lack of routine: no/little set daily routine, frequent travel Alcohol consumption (any)
Factors associated with non-adherence Ekstrand et al. under review
Understanding medication adherence barriers: Focus group data n=17 males & 13 females reporting adherence challenges Perceptions of stigma and fear of discrimination prevented patients from disclosing their HIV+ status. Unable to ask others for help remembering doses. Problems explaining frequent clinic visits to family and employers & getting help with transportation. Lack of privacy interfered with taking pills in front of others, especially during holidays/family gatherings. Patients did not want to fill their prescriptions at the local pharmacy, due to lack of confidentiality.
The role of stigma in adherence Occasional missed pills Forgetfulness Lack of privacy Worksite issues Travel/holidays Treatment failure & resistance Lack of disclosure No/little social support Fear of stigma Treatment interruptions No time off work Clinic transportation Accessing local pharmacy
Conclusions Ongoing adherence levels comparable to other international settings Treatment interruptions most common form of non-adherence, most often associated with delays in prescription refills Non-adherence –especially in the form of treatment interruptions - are associated with both viral load and resistance mutations To improve treatment outcome and minimize the development of resistance, barriers to uninterrupted treatment must be addressed! AIDS stigma is a crucial factor underlying both occasional missed doses and treatment interruptions. Needs to be targeted in adherence interventions at the level of the individual, family, institutions, and society
THANK YOU! Prerana Study TeamSt John’s Research Institute, Bangalore




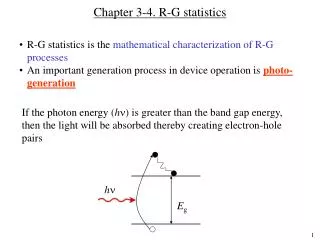
![[HAuCl 4 ] (M)](https://cdn1.slideserve.com/3094085/slide1-dt.jpg)