Download
1 / 45
450 likes | 642 Views
The Effect of UNHS on Early Cochlear Implantation. Antonia Brancia Maxon, Ph.D. Diane Brackett, Ph.D. Jennifer Cox, M.A. Alicia Ayles, M.A. New England Center for Hearing Rehabilitation. Why is Early Identification of Hearing Loss so Important?.

E N D
The Effect of UNHS on Early Cochlear Implantation Antonia Brancia Maxon, Ph.D. Diane Brackett, Ph.D. Jennifer Cox, M.A. Alicia Ayles, M.A. New England Center for Hearing Rehabilitation NECHEAR
Why is Early Identification of Hearing Loss so Important? • Congenital hearing loss interferes with the most basic human need to communicate with others • Hearing loss is the most frequent birth defect • Undetected hearing loss has serious negative consequences • There are dramatic benefits associated with early identification of hearing loss NECHEAR
UNHS lowers age of intervention • Infants with hearing loss should be fit with hearing aids by four months old • Infants with hearing loss should be enrolled in early intervention by four months old NECHEAR
UNHS lowers age of intervention • When a six month hearing aid trial is used • Benefit from traditional amplification can be determined by 10 months old • Infants who do no benefit should not have to wait for the implant. NECHEAR
UNHS affects the age of cochlear implant candidacy identification • Until recently the recommended age of implantation was 18 months old. • Now 12 months is recommended lowest age. • Surgeons are implanting even younger infants. NECHEAR
Early Identification Ensures Some Critical Criteria Are Met • Objective measures are available to make a diagnosis within the first month of life. • will know degree of hearing loss • will know the configuration of hearing loss • will know if there are middle ear problems • Can begin process of candidacy evaluation NECHEAR
Early Identification Ensures Some Critical Criteria Are Met • Parents have accepted the hearing loss and are ready to begin appropriate intervention. • Parents are aware of communication modality options. • Parents know the role of and need for sensory devices. NECHEAR
Candidacy • Bilateral severe to profound sensorineural hearing loss • Infant/toddler cannot benefit from traditional amplification NECHEAR
Diagnosis to Decision - Parent • Need to understand: • no device is a cure • therapy is long-term • language learning is an ongoing process • access to acoustic speech cues • how access relates to child’s progress NECHEAR
Diagnosis to Decision - Parent • Need to: • understand the difference between reacting to cues received through hearing and other senses • identify auditory responses • learn how to use the home, family, environment in a positive way for auditory and language learning NECHEAR
Diagnosis to Decision - Parent • Need to be comfortable with equipment • know how to use it properly • know how to modify clothing to accommodate it • accept that people will look, question, comment on it • able to troubleshoot equipment and child’s auditory behavior NECHEAR
Diagnosis to Decision - Parent • Need to understand the audiogram • know the degree and configuration • know the basics of acoustic cues of speech • know how speech perception is affected by their child’s hearing loss • know what their child actually receives NECHEAR
Diagnosis to Decision - Child • Child needs to be fit with best amplification • must get the most auditory stimulation possible • body-worn FM system • snap-on transducers • power transducers • earmolds - good fit at all times NECHEAR
Diagnosis to Decision - Child • Child needs to be enrolled in an EI program that stress auditory function • learning to use hearing • learning to respond to sound • learning to respond to speech • learning the need for communication NECHEAR
Assessing Auditory Function • From initial enrollment in EI always assessing auditory function • Should not make decision about hearing aid or cochlear implant based on pure tone audiogram • Need to determine if child is able to make maximal use of residual hearing NECHEAR
Assessing Auditory Function • Child needs to receive speech at an appropriate level with amplification • detection is not enough • have to look across frequencies for access to all speech sounds • speech needs to be received at a useable level NECHEAR
Assessing Auditory Function • Child must have good access to speech of others and own speech • at different distances from sound source • Child should alert to a variety of speech and non-speech sounds • at different distances from sound source NECHEAR
Assessing Auditory Function • Child’s output • vocalization • precursor to speech production • intentional vocalization • precursor to language • vocalization + gesture • intention to communicate NECHEAR
Indications the Child is a Candidate • Child shows limited or no detection of amplified speech • Comparisons of audiological data and functional use of hearing • Knowledge of the child’s auditory limitations NECHEAR
Factors that Facilitate CI Success • Parents know about hearing loss and accept long-term problems • Parents understand the implant is not a cure • Parents are committed to implant use • Parents are committed to therapy NECHEAR
Factors that Facilitate CI Success • Family has access to therapy and mapping facilities • Family is motivated • One parent at home - minimal day care • The household is organized • Child is vocalizing • Child has normal cognitive level NECHEAR
Absence of one or more of those facilitating factors does not rule out the child’s candidacy. NECHEAR
Why Implant Early • Critical period of communication development • Children implanted below 10 years old • children implanted before age 3 showed a greater period of auditory plasticity • open-set speech recognition could not be achieved after 6 years old (Manrique, et al, 1999) NECHEAR
Why implant early? • Early is better for children with hearing aids (Apuzzo & Yoshinaga-Itano, 1995) • Early implantation • allows for extended listening time before social and school demands start • decreases chance of a large gap between chronological and communication age • promotes acquisition of speaking and language NECHEAR
Why implant early? • Children implanted early (2-3 years) make greater growth than later implanted (3-5 years) children • expressive vocabulary • receptive vocabulary • dramatic improvements first year post implant (Brackett and Zara, 1998) NECHEAR
Why implant early? • Surgical risks are minimal • Complications are infrequent • Objective testing can be used to predict appropriate programming • Can use audiological behavioral measures for programming (Cohen, Drous, Shapiro & Waltzman, 2003) NECHEAR
Information Needed by Parents • Parents wanted most information prior to surgery, but wanted continued informational support post-implant • Parents felt emotional support was most lacking • Majority of parents felt there needed to be a professional liason between CI center and educational program (Most and Zaidman-Zait, 2003) NECHEAR
Cochlear Implant Surgeon Selection • Competent and experienced with infants • Familiar with surgical placement of receiver/stimulator package that reduces potential damage from head impact NECHEAR
Cochlear Implant Surgeon Selection • Familiar with techniques that reduce intracranial complications • Willing to make accommodations for child and family regarding hospitalization, pre- and post-surgery conditions NECHEAR
Mapping Audiologist Selection • Competent and experienced with infants • Familiar with VRA • Availability of multiple testers • Availability of appropriate equipment and reinforcement NECHEAR
Mapping Audiologist Selection • Knows about speech acoustics • Uses functional measures to fine tune the map • Accepts input from parents and rehabilitation professional • Maps the implant “on demand” • Knows about aural rehabilitation NECHEAR
Surgery to Stimulation • Child • becomes familiar with and gets used to equipment • uses hearing aid on non-implanted ear • Aural rehabilitation • communication focus continues • conditioning sessions to facilitate mapping NECHEAR
Initial Stimulation • Short term goal is good access to speech across frequencies • Weekly sessions until have a good map • Use input from parent(s) and rehabilitation professional • Use functional responses to modify maps NECHEAR
Rehabilitation Professional Selection • Knowledgeable about: • infant behavior • infant development • infant communication • auditory development • activities that facilitate auditory-vocal behavior NECHEAR
Rehabilitation Professional Selection • Knowledgeable about: • infant adaptation to equipment • home therapy suggestions • troubleshooting the equipment • troubleshooting the child’s behaviors NECHEAR
Rehabilitation Programming • Keeping external components on head • Keeping body processor comfortable • Continued conditioning for mapping when necessary • Mapping as required • parent request • rehabilitation professional request NECHEAR
Case Study - Stevie • UNHS - failed bilaterally (before mandate in CT) • Bilateral profound SNHL diagnosed - 5 mos • Hearing aids fit - 5 mos • Enrolled EI (2x/week) - 6 mos • FM fit - 10 months NECHEAR
Case Study - Stevie • Aided response levels - 50-60 dB HL • Aided SAT - 45 dB HL • CI evaluation - 10 mos • CI surgery - 13 mos • Initial stimulation - 14 months NECHEAR
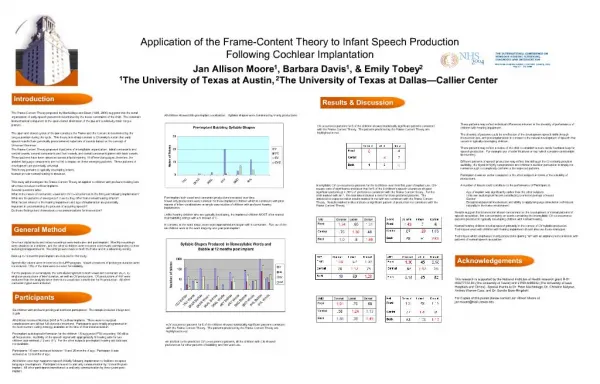
Case Study - Stevie(evaluation at 32 months) • Speech perception: 100% spondees, 83% monosyllables • Speech production: 75% consonants, 97% vowels • Vocabulary: Receptive - not basal, Expressive - <1.9 years • Utterances: 4-5 words, not many verbs, rising inflection for questions NECHEAR
Case Study - Stevie(evaluation at 46 months) • Speech perception: 100% consonants, 100% vowels • Speech production: 90% consonants, 100% vowels • Vocabulary: Receptive - 10 month delay, Expressive - 8 month delay • Sentences: 5-7 words, nouns and verbs some adjectives, possessive, plural markers emerging, some pronouns. NECHEAR
Case Study - Anna • UNHS - failed bilaterally (post mandate) • Bilateral profound SNHL diagnosed - 3.5 weeks • Hearing aids fit - 4 weeks • Enrolled EI (2x/week) - 4 weeks • Hearing aids and FM fit - 4 weeks NECHEAR
Case Study - Anna • Aided response levels - 40-50 dB HL • Aided SAT - 35 dB HL • CI evaluation - 10 mos • CI surgery - 11 mos • Initial stimulation - 12 months NECHEAR
Case Study - Anna(evaluation 28 months) • Speech perception: excellent • Speech production: errors - m/n, g/d, omits ch, t, m, z • Vocabulary: Receptive - 21 months, Expressive - 21 months • PLS: Auditory Comp - 31 months, Expressive Comp - 28 months, Total Language - 30 months NECHEAR
Universal Newborn Hearing Screening • Lowers the age of hearing loss diagnosis • Lowers the age amplification is provided • Lowers the age of enrollment in early intervention • POTENTIALLY lowers the age of cochlear implantation NECHEAR
Benefits of Early Cochlear Implantation • Minimizes the effects of auditory deprivation • Electrical stimulation provides necessary information to auditory system at critical period for speech and language acquisition. • Provides child with a good chance to develop normal speech and language NECHEAR