Download
1 / 24
240 likes | 281 Views
Learn about the epidemiology, assessment, associated injuries, radiographic evaluation, and management of pelvis fractures, including specific patterns and related anatomical considerations.

E N D
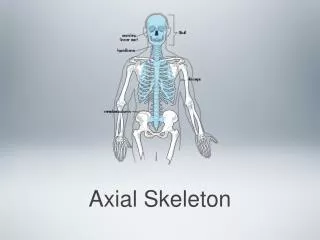
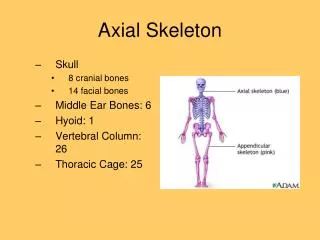
Common adult fracturesAxial skeleton (Pelvis) Waleed M. Awwad, MD. FRCSC Assistant professor and Consultant Orthopedic Surgery department
Epidemiology • 37 cases per 100,000 / year at USA. • Age: • Young: high energy mechanisms. • Elderly: minimal trauma. • Male are more commonly affected before the age of 35.
Pelvic stability • Rotational or vertical. • Sacroiliac displacement 5mm. • Posterior fracture gap. • Symphysis diastasis. • Specific injury pattern (direction of force): • AP external rotation of hemipelvis, spring open. • LC (T-bone): • Posterior half of ilium. • Anterior half of iliac wing. • Greater trochanteric region. • External rotation and abduction, shear forces.
Assessment • ABCDE’s must be assessed first and treated appropriately. • Patients should be examined with spinal collar until spinal pathology is excluded. • Careful log rolling keeping the head, neck and pelvis in line should be done to examine the spine properly. • Pelvic stability test (AP-LC only once). • Massive flank or buttock contusion. • Palpation of posterior aspect, symphysis and perineum. • Digital rectal and vaginal exam in any pelvic ring fractures.
Assessment • Hemodynamic status: • Usual cause of retroperitoneal hemorrhage is venous. • Arterial bleeding: • Small vessels: embolization • Large vessels: immediate surgical exploration. • At emergency: open book pelvic fracture. • Pelvic wrapping at the level of GT.
Associated injuries • Neurological: Lumbosacral plexus and nerve root. • Genitourinary: • Bladder: 20% incidence. • Extraperitoneal: foley if unable to pass. • Intraperitoneal: surgical repair. • Urethral:10% incidence. male > females. • Blood at meatus or catheterization, high ridding prostate. • Any clinical suspicion retrograde urethrogram. • Bowel: perforation (open injury), rarely entrapment. • Diverting colostomy.
Radiographic evaluation • AP pelvic view. • Inlet and outlet views. • Obturator and iliac oblique views if acetabular fracture. • Computed tomography. • MRI (limited clinical utility).
Management • Depend on severity and stability.
Management • Depend on severity and stability. • If stabile: protected weight bearing and serial X-rays. • If unstable: • External fixation. • Internal fixation. • Absolute surgical indication: • Open pelvic fractures. • Open book pelvic fracture or vertical unstable.
Acetabulum • 3 per 100,000 population / year. • Neurological injury up to 30% (peroneal division more than tibial). • Components: • Anterior and posterior column. • Acetabular dome (weight bearing area).
Radiological • Obturator and iliac oblique views: • Iliac oblique: posterior column, iliac wing and anterior wall of the acetabulum. • Obturator oblique: anterior column and posterior wall of the acetabulum.
Management • Goal of treatment is anatomic restoration of articular surface to prevent post traumatic arthritis. • Non operative treatment: • Non displaced fracture or less than 2mm displacement. • Less than 20% posterior wall fracture. • Surgical treatment: • Displacement >2mm. • Large posterior wall fragment. • Intra-articular fragment. • Irreducible fracture dislocation. • Posterior instability.