Download

1 / 47
480 likes | 559 Views
Quality Improvement in the Retail Setting. Stan Jeppesen, Pharm.D. Washington State Board of Pharmacy. Objectives. Provide an introduction into flow chart analysis Identify simple processes for monitoring system integrity and identifying opportunities for process improvement

E N D
Quality Improvement in the Retail Setting Stan Jeppesen, Pharm.D. Washington State Board of Pharmacy
Objectives • Provide an introduction into flow chart analysis • Identify simple processes for monitoring system integrity and identifying opportunities for process improvement • Identify basic principles of a PDSA (Plan, Do, Study, Act) cycle
Objectives • Review basic principles of Continuous Quality Improvement (CQI) that apply to conducting PDSA cycles and data collection • Provide a simple examples of two PDSA cycles • Identify how the PDSA cycles can be applied in the retail setting
Basic Concepts • Flow charts: • Describes the system • Identifies the opportunities to be found • PDSA: • Provides a simple, safe way to make small incremental changes • Identifies the impact of the change • Management: • Deals with FEAR so projects will be successful
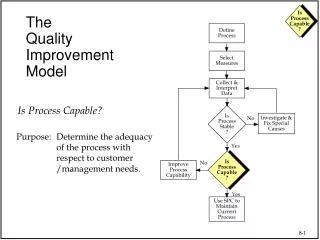
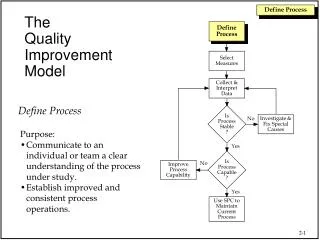
What is a flow chart? • Flow charts are a step-by-step schematic picture used to describe a process being studied • Flow charts can be augmented with additional written and/or schematic descriptions of the individual processes
What does it do for you? • Provides common reference points • Standard language to use when talking about an existing process • Describes new improved system(s).
What does it do for you? • It allows you to easily describe an entire process • Allows for identification of processes and procedures • It is a powerful communication tool
Why Use It? • To help identify the root cause of a problem • To help Identify opportunities for improvement(s)
Reference Attachments • See example flow chart attachments • See example data collection tools
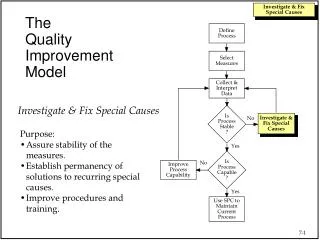
The PDSA Cycle Act Plan Study Do
What is the PDSA Cycle? • Act • What changes are to be made? • What is the next cycle? • How do we hold the gains • Plan • Objective • Questions and predictions (why) • Plan to carry out the cycle (who, what, where, when, How) • Study • Complete analysis of the data • Do • Carry out the Plan • Collect the data • Document problems and unexpected observations • Begin data analysis • Compare data with predictions • summarize what was learned
Provide objective information Increase info about the change (Positive/negative) Give some expectation of the change impact Show if the gains are retained Involve the staff in the changes Provide economic impacts Reasons for Collecting Data
Model for Improvement What are we trying to accomplish? How will we know that a change is an improvement? What change can we make that will result in improvement? Act Plan Study Do Source: Inst. For Healthcare Improvement, “IHI Quality Improvement Resources: A Model for Accelerating Improvement,” Boston, MA: Available at WWW.ihi.org/resources/qi/.
Aim: Improve Counseling Frequency Improved Counseling Frequency p A D S Minimize the number of medication errors leaving the Pharmacy Cycle 5: Train additional Pharmacists. A S P D Data Cycle 4: Revise the tracking system to use a paper receipt. A P S D A S P D Cycle 3: Orient one Pharmacist to the counseling tracking. Increase the number of Patients counseled. Cycle 2: Revise the counseling tracking using paper clips and train two Techs. A P S D Cycle 1: Devise and test a system to track the number of patients counseled.
Aim: Minimize medication errors Improved Rx Accuracy p A D S Minimize the number of medication errors passing through the filling process Cycle 5: Give staff feedback on scanner stats and errors. A S P D Data Cycle 4: Orient other Pharmacists to Scanner use. A P S D A S P D Cycle 3: Orient one Pharmacist to the scanner in the new location. Utilize the Scanner for process control during the prescription filling operations. Cycle 2: Try out the new location during the filling process yourself. A P S D Cycle 1: Test out the new location of the scanner yourself.
Management’s Role • Management role to optimize the system as a whole • Win-Win for Patients, Physician, Family, organization • Meet the patient needs • Deliver top quality services • Institute Training • Improve constantly • CQI Starts at the Top
Dealing with Fear • Employees/Staff are intrinsically motivated • Performance rating can often be destructive • Employees often blamed for “System Problems” • Fear Stifles the human contribution • Lack of reporting - Cover up info • Distort information - Inhibits questions • Restrains expression and ideas
Implement a non-blame Environment • To help reduce FEAR • Increase participation • Increase data quality and reporting • Increase the success of the quality projects
Summary • Flow charts: • Describes the system • Identifies the opportunities to be found • PDSA: • Provides a simple, safe way to make small incremental changes • Identifies the impact of the change • Management: • Deals with FEAR so projects will be successful
Summary • Keep it simple • Make it easy • This is Not Hard • Keep it a learning experience • Have fun with it
Questions? • Stan Jeppesen, Pharm.D. • Investigator for the Washington State Board of Pharmacy • Stan.Jeppesen@doh.wa.gov • (206) 528-0732 Seattle Office
References • Kohn LT, Corrigan JM, Donaldson MS. To Error is Human. Institute of Medicine, National Academy Press 1999. • Institute for Healthcare Improvement, BMJ Publishing Group. www.QualityHealthCare.org • Juran JM. Juan on Quality by Design. The Free Press, 1992. • Deming WE. Out of the Crisis. Cambridge, MA; MIT Press 1986. • Pharmacists Quality Improvement Project I, February 21, 2002. Qualis Health. www.qualishealth.org • Pharmacists Quality Improvement Project II, March 14, 2003. Qualis Health. www.qualishealth.org
When an Error Occurs • What do you do?? • What does the patient want? • What is your liability? • How do you handle it?
When an Error Occurs -What do you do? • Complete an error report? • Admit no guilt or participation? • Determine the cause or who? • Hope the incident goes away?
What does the patient want? • An acknowledgement of the error • An admission of guilt • An admission of alarm over the potential harm • That the cause will be fixed and not repeated • That they or someone else won’t get hurt in the future
Why do patient report errors • No sense or admission of caring • Fear that “they” will do it again and hurt someone • Denial by the staff that they made a mistake • No apology • It has occurred twice before • They made it appear to my fault
What is Your Liability? • Has the patient been injured? • Did the patient suffer a financial loss?
What are we afraid of? • Lawsuits ? Legal Liability ? • Lower the Patient trust..? • Disclosure of embarrassing situation? • Revealing a personal failure? • Self-esteem • ?
What should patient be informed of? • What happened • What the error was • Why error happened • What has been learned –how it will be prevented • How sorry you are…the apology