Download
1 / 24
240 likes | 335 Views
Are Drug Pricing Formulas Full Employment Acts For State Attorney Generals?. Gerard Anderson PhD Professor Johns Hopkins University. Lake Wobegon Syndrome : How Can Everyone Be Getting A Better Deal?. U.S. vs. Other Countries Medicaid vs. Other Payors Maryland vs. California

E N D
Are Drug Pricing Formulas Full Employment Acts For State Attorney Generals? Gerard Anderson PhD Professor Johns Hopkins University
Lake Wobegon Syndrome : How Can Everyone Be Getting A Better Deal? • U.S. vs. Other Countries • Medicaid vs. Other Payors • Maryland vs. California • Maryland Medicaid vs. Maryland Prisons
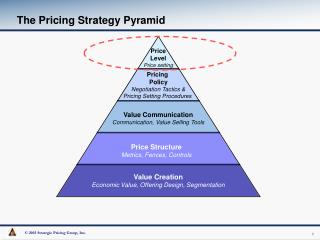
Economics 101 – Fixed vs. Variable Costs • Fixed Costs • costs that must be incurred regardless of number of units sold • Variable Costs • costs of producing one additional unit • Examples • Fixed - plant and equipment or R & D • Variable - materials
Standard Economic Theory – Price Determined By Where Variable Cost is Lowest - Fixed Costs are Irrelevant Firms Produce Where Variable Cost is Lowest
In Reality –Fixed Costs Matter Pharmaceutical companies could not exist if everyone only paid only the variable cost
Most Pharmaceutical Spending Involves Fixed Costs • Marketing: 32.8% • Costs of Goods Sold: 25.3% • Profit: 20.6% • R & D: 14% • Taxes: 7.3%
$64,000 Policy Question • Who should pay the fixed costs of pharmaceutical companies? • U.S. vs. other counties • Medicaid vs. other payors • Maryland vs. California • Maryland Medicaid vs. Maryland Prisons
Who Is Paying The Fixed Costs? • U.S. pays twice as much as other countries • Almost 2 to 1 difference in government payors: • Medicare • 340 B • Medicaid • VA • DoD • Some states pay 3 times what other states pay • Significant variation within state programs
Policy Issue – Spillover Effects • If payor (e.g. Medicaid) gets a lower price then will other payors have to make up the difference? • One economic assumption: • Pharmaceutical companies will be able to raise prices to other payors (programs) to cover their fixed costs • Alternative economic assumption: • Each payor (program) negotiates the best price independently of what other payors (programs) pay
My Perspective On Spillover Effects • Each pharmaceutical executive will want to maximize the revenue from each payor (program) • Result is that states need an economic not just a legal rationale for getting low drug prices
Full Employment for Attorney Generals • Without an economic rationale companies will try to maximize revenue in Medicaid by “gaming” the system
Unlike Most Goods and Services the Consumer Is Not King In Pharmaceutical Pricing • Physicians must prescribe drugs • Hospitals, nursing homes, HHAs use formularies • Pharmacies can push drugs that earn them greater profits • Patients pay small portion of bill out-of-pocket
Remember the Spread • Spread is the difference between pharmacy (hospital, LTC, HHA) purchase price and what Medicaid believes is the purchase price • In 2002 CBO calculated that pharmacies earned the following spreads in Medicaid • 23% overall • 30% generics • 14% brand names
What Are The Economic Incentives? • Drug companies want pharmacies to earn the most money on their drugs so they will prescribe them • Pharmacies will want to prescribe drugs that earn them the most money • Both drug companies and pharmacies benefit when the spread is greater • Medicaid loses when the spread is larger
Trust Me I Am From Pharma • The source of all the pricing data is the pharmaceutical companies • AWP, AMP, ASP, EAC, FUL, MAC, WAC
AMP and Best Price • Average Manufacturers Price (AMP) is supposedly what a drug company receives for a drug in a given quarter from retail pharmacies • Best price is supposedly the lowest price in retail pharmacies • Medicaid rebates are determined based on difference • How can any state validate either best or AMP?
Auditing • CMS investigated pharmaceutical company reported data on only 4 occasions over a 10 year period according to GAO
Lake Wobegon • Rebates are difficult to monitor when the pharmaceutical industry has all the data • Not every state can be getting the best deal • Some states pay almost 5 times more for the same drug
Price Transparency • Find out the actual prices other payors are paying for the same drugs • U.S. vs. Other Countries • Medicaid vs. Other Payors • Maryland vs. California • Maryland Medicaid vs. Maryland Prisons
Comparative Data Allows A Bully Pulpit • With comparative price data states can see where they are getting a good deal and when they are paying higher prices • Must be done on a drug by drug basis • States can then focus their negotiations on the prices of drugs where they pay much higher prices
Conclusion • Who is going to pay the fixed costs of the pharmaceutical industry? • Gaming will occur without an economic rationale for discounts and rebates • Cannot rely on pharmaceutical companies for all the data to determine prices • Price transparency will tell states when they are getting a good deal