Download
1 / 17
190 likes | 377 Views
CHICKENPOX (VARICELLA). VZV. The Varicella-Zoster Virus (VZV) belongs to the HERPES group. Pathogenic only for man; occurs worldwide . Causes 2 distinct clinical patterns: primary and latent.

E N D
CHICKENPOX (VARICELLA) DR (MRS) M.B. FETUGA
VZV • The Varicella-Zoster Virus (VZV) belongs to the HERPES group. • Pathogenic only for man; occurs worldwide . • Causes 2 distinct clinical patterns: primary and latent. • The primary infection is manifested as varicella (chickenpox) and results in establishment of a lifelong latent infection of sensory ganglion neurons. • The reactivated infections are known as herpes zosters (shingles). • It is predominantly a disease of childhood in tropical Africa. • Varicella is highly infectious in children. DR (MRS) M.B. FETUGA
PATHOGENESIS 1 • Infection is spread by direct contact and by air droplets. • The virus may be contained in the pharyngeal secretions hence the infectivity via air droplets. • Patients are infectious for 2 days before the appearance of the rash and until the skin lesions have crusted although the crusts do not usually contain viable viruses. • The viruses gain entry via the mucosa of the conjunctivae, nasopharynx and URT. DR (MRS) M.B. FETUGA
PATHOGENESIS 2 • Viral replication takes place at the point of entry and they invade through the local lymphatic and blood vessels resulting in viraemia. • At this stage, the viruses are seeded in the dorsal root ganglion cells where they remain dormant even after the acute infection has resolved. • Antibodies are formed which protect against re-infection but not against re-activation of latent infections. DR (MRS) M.B. FETUGA
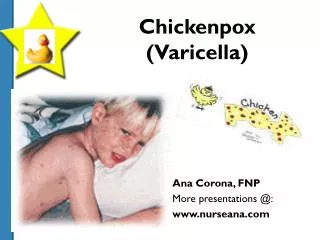
CLINICAL FEATURES OF VARICELLA • Diagnosis- clinical • VARICELLA begins usually SUDDENLY after an IP of 14 – 17 days. • Rash is usually accompanied by fever, malaise and pruritus. • Rash 1st appears on scalp & face and spreads to the trunk. Distribution is typically centripetal (more on the trunk than on the limbs; but spares hands & soles of feet). • Lesions begin as macules then turn to papules and vesicles. They crust within 2-3 days. DR (MRS) M.B. FETUGA
Chickenpox rash with blisters, pustules & scabs DR (MRS) M.B. FETUGA
CLINICAL FEATURES OF VARICELLA • New vesicles continue to appear over the first week of the illness. Typically, the rashes are present in different crops at the same time. • In Atypical form- the rash is not characteristic in appearance & distribution. The rash involves the flexural areas and concavities like the axillae, groin and mucous membranes of the nasopharnyx, conjunctivae & cornea. • Healing is usually complete although very minimal scarring may be present unlike in smallpox where scarring is massive. DR (MRS) M.B. FETUGA
CLINICAL FEATURES OF VARICELLA • The rash involves the flexural areas and concavities like the axillae, groin and mucous membranes of the nasopharnyx, conjunctivae & cornea. • Healing is usually complete although very minimal scarring may be present. DR (MRS) M.B. FETUGA
COMPLICATIONS OF VARICELLA • Generally benign in children with low mortality & few complications but may be fatal in neonates • Complications usually occur in debilitated and immunocompromised children, particularly those with: TB, severe malnutrition, Measles, HIV, malignancies and steroid therapy. • Secondary skin infection by Staphylococcus and Streptococcus. • CNS (due to post-infectious demyelination). e.g. encephalitis (cerebellar in form), polyneuritis, transverse myelitis and Reye syndrome. DR (MRS) M.B. FETUGA
COMPLICATIONS OF VARICELLA • keratitis,conjunctivitis, carditis, appendicitis, glomerulonephritis, orchitis • DIC- thrombocytopenia DR (MRS) M.B. FETUGA
CLINICAL FEATURES OF ZOSTER • Zoster is uncommon in childhood. • Early onset dx more likely to be ffged by herpes zoster due to persistence & prolonged presence of virus in the body • It is heralded by pain in the affected dermatome. • Few days later, the rash appears along the painful dermatome: typically, unilateral, segmental and proximal. • Any cranial or spinal sensory nerve may be affected but the thoracic nerves are most frequently affected. • The rashes are similar to those of varicella but are deeper and tend to heal with scarring. DR (MRS) M.B. FETUGA
NEONATAL VARICELLA • Most babies acquire protective antibodies transplacentally, hence they are protected for the first 6 months of life (ONLY IF THE MOTHER PREVIOUSLY HAD THE INFECTION AND FORMED ANTIBODIES) • If a susceptible mother develops varicella rash 7 days or less before delivery, NEONATAL VARICELLA may occur in the baby. If the mother develops the rash more than 7 days before delivery, there is adequate time for the synthesis and transfer of antibodies against the virus. • Affected babies usually manifest 5-10 days after birth. • Mortality in Neonatal Varicella: 10 - 20%. DR (MRS) M.B. FETUGA
CONGENITAL VARICELLA • Follows maternal varicella in the first 2 trimesters. • Xterised by multiple congenital anomalies including choroiditis and cerebral malformation. • Features include: skin scars, contractures, hypoplastic limb deformities with rudimentary digits, congenital cataract and microphthalmia. DR (MRS) M.B. FETUGA
MANAGEMENT • Diagnosis is usually clinical. • Viral culture & serology may be done where facilities are available. • Treatment is largely symptomatic: calamine lotion to soothen the skin, oral antihistamines like promethazine and analgesia with paracetamol. • Secondary bacterial infection of skin lesions can be treated with topical silver sulphadiazine or chlorhexidine. Systemic antibiotics are only indicated when cellulitis occurs. • Post-exposure prophylaxis with IM Varicella-Zooster Immunoglobulin 2mL confers about 97% protection. • Clinical trials of a live attenuated vaccine are being done. DR (MRS) M.B. FETUGA
PROGNOSIS • Recovery is ffged by long immunization. 2nd infection occasionally occurs DR (MRS) M.B. FETUGA
PREVENTION • Vaccine - available, safe & effective. • Mainly used for children about to be treated with immunosuppressive drugs (leukemia) DR (MRS) M.B. FETUGA
DIFFERENTIAL DIAGNOSIS • Impetigo, scabies, dermatitis multiforme DR (MRS) M.B. FETUGA