Download
1 / 30
300 likes | 428 Views
Elements of Health System Financing Lecture 3 of 6. Allocation of Resources in the Health System. Objectives of Third Lecture. Revisit the concept of ‘ Allocation ” Delineate different dimensions of allocation and identify options Describe the fundamental features of the different options

E N D
Objectives of Third Lecture • Revisit the concept of ‘Allocation” • Delineate different dimensions of allocation and identify options • Describe the fundamental features of the different options • Discuss how well each option serves different aims of the health system.
Structure of Lecture • Review and introduction • Characteristics of different allocation options • Ranking of forms of allocation and recipient institutions by their potential impact on relevant health system aims • Summary.
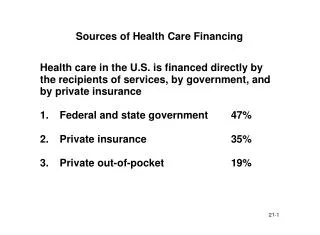
Reminders • We are in the ‘public domain’: universal or categorical ‘public entitlement’ is secured through revenues raised using public finance principles • “Level” and “Sources” of finance are the subject of macro-economic policy, determined mostly outside the health system • “Allocation” (with “Payment to Providers”) is the subject of health policy, determined mostly within the health system • The ‘contributors’ to the system are not necessarily the ‘beneficiaries’ • Beneficiaries are by and large entitled only to services are in kind • The agency that raised funds for medical care needs to secure services for the beneficiaries
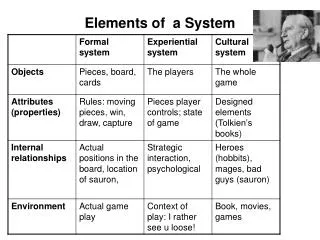
The Basic Matrix: Health System Aims Vs. Financing Elements, Not Including “Level” and “Health”)
The Options to Secure Service • Direct purchase from providers • Contracting and intermediary: • Region • OMCC – organization that manages the consumption of care • A combination of the two • These reflect the administration of the system, the nature of its decentralization, and its implicit or explicit priorities --- mirrors the health system
The Concept of Allocation • Allocation –the mechanism or part thereof to secure the parameters or envelop of public entitlement • Related to the concepts of • ‘purchasing’ • ‘contracting’ • Is closer to ‘contracting’ in that the contracted entity is doing the purchasing…
Contracting / Allocation Institutional Scheme – The Commonwealth / NHIS Model State Funding Budget Contracting –Administration -NHS Purchasing Providers
Contracting / Allocation Institutional Scheme – The “Continental” /OMCC Model State Regulation Funding Pool Real or Virtual Contracting OMCC institutions: Sickness Funds, HMOs Purchasing Providers
Dimensions of Allocation • Objectives or criteria of allocation • Forms of allocation • Recipient institutions • We focus on the first two
Forms or Options of Allocation • Vouchers • Budgeting • Prospective capitation • Retrospective capitation.
Criteria for Ranking Forms of Options • Equity: • Willingness of “contractor” to deal with specific needs • Macro-economic efficiency: • Ability of system to withstand ‘upward’ pressures to increase cost of care • Micro-economic efficiency • The incentive of the contractor to save on cost of service, given quality • Client satisfaction • The incentive of the contractor to look for clients and satisfy them by at least quality of service, if not care
Potential Impact on Macro-Economic Efficiency or Cost Containment –(Ordinal Ranking)
Potential Impact on Micro-Economic Efficiency–(Ordinal Ranking)
Potential Impact of Forum of Allocation – Summary(Ordinal Ranking)
Options for Recipient Institutions • Regional or local administrations (e.g., health regions or districts in the UK, or for that matter, states in federal systems); • OMCC institutions of different types (e.g., HMOs in the US, and sickness funds in the Netherlands and Israel) • ‘Budget holding’ general practitioners and clinics (as in GP budget holding in the UK) • Options are not mutually exclusive
Potential Impact on Macro-economic Efficiency–(Ordinal Ranking)
Potential Impact on Micro-economic or Production Efficiency –(Ordinal Ranking)
Potential Impact of Allocation by Recipient – Summary (Ordinal Ranking)
What Next? Provider payment mechanisms