Download
1 / 17
380 likes | 1.14k Views
AKI (formerly ARF). 13–18% of all people admitted to hospital. Format for the Session. 8.10 Acute Kidney Injury (AKI) R ecognise AKI/potential for AKI Distinction from chronic renal failure Establish underlying pathophysiology (causes) Investigations Management P rognosis

E N D
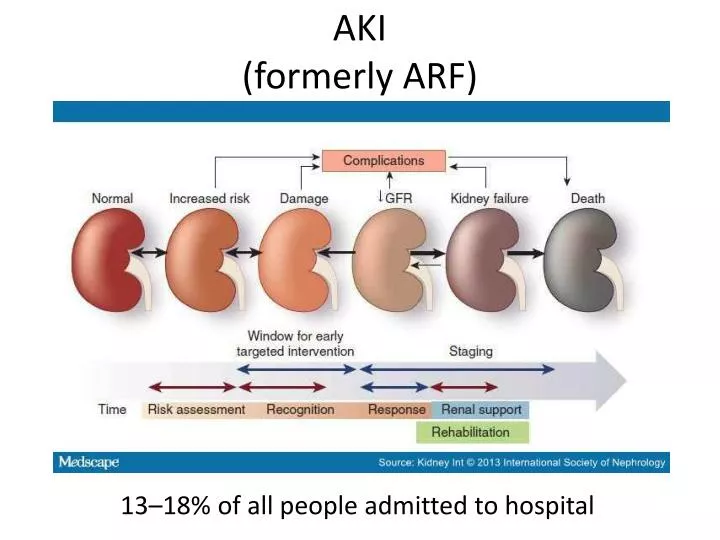
AKI(formerly ARF) 13–18% of all people admitted to hospital
Format for the Session 8.10 Acute Kidney Injury (AKI) • Recognise AKI/potential for AKI • Distinction from chronic renal failure • Establish underlying pathophysiology (causes) • Investigations • Management • Prognosis • Prevention
Recognise (Potential) Acute Kidney Injury Within the past 7 days: • sCr rise of 26 micromol/l + in 48 hrs • 50% + rise in sCrknown or presumed to have occurred • urine output <0.5 ml/kg/hr for 6 hrs+ • NB children differ!
Causes of AKI 50% of AKI
Investigation of AKI Bedside tests • Strict urine output monitoring with catheter (if not already) • Dip, urine osmolarity, MCS • Weight BD • ECG Bloods • Lactate • Serial sCr, Urea, electrolytes, serum osmolarity • Cultures Imaging • USS within 24hrs IF pyonephrosis(infected and obstructed kidney[s]) is suspected • Chest Xray Special
Initial Management of AKI Pre Renal • Stop nephrotoxics, do not use loop diuretics to force urine output • Rehydrate, correct electrolytes, treat sepsis with ?kidney friendly Abx Renal • Call nephrology (NICE say so!) Post Renal • Acute retention catheterise • Ureteric obstruction ?Nephrostomy Urology
AAAAAH my treatment is not helping!! When there’s something bad, and it don’t look good Who yagonna call?
Your SHO/reg and suggest a referral to Renal boffins for an opinion on haemodialysis
Indications for dialysis(usually haemofiltration in ITU) • Known Tx/dialysis patient OR • Initial treatment failure AND one of AEIOU
What’s AEIOU you say?!! Acidosis (metabolic)Electrolyte changes (hyperkalemia)Ingested Toxins (barbiturates, salicylates, lithium, methanol)Overload (pulmonary oedema unresponsive to diuretics)Uremia symptoms (pericarditis, encephalopathy)
Triggers to call the nephrologist in the 1st Instance • Initial treatment measures fail • Specialist diagnosis (vasculitis, glomerulonephritis, tubulointerstitial nephritis or myeloma) • AKI cause not clear • AKI has caused complications • Stage 3 AKI (according to (p)RIFLE, AKIN or KDIGO criteria) • Transplant/ CKD stage 4 or 5 patient
Prognosis of AKI • 20-30% mortality and increasing with each stage of AKI • Risk of CKD • 15-32% of survivors are dependent on RRT at hospital discharge • Nephrology Follow Up
Prevention • Older adults, comorbidities, surgery, contrast studies • Do NOT perform a contrast investigation without a U&E’s • Avoid nephrotoxic meds as far as poss and stop ACE/ARB pre-contrast (pharmacist) • Consider preloading with N.Saline • Avoid dehydration, particularly before surgery
References • http://www.fastbleep.com/ • NICE clinical guideline 169 guidance.nice.org.uk/cg169
kidneys receive 20-25% of the resting cardiac output via the right and left renal arteries • 1. Cardiac output which determines the amount of blood flow down the renal arteries • 2. Autoregulationwhich sets the pressure gradient between the afferent and efferent arterioles; and • 3. Size and charge of molecules that are going to be filtered through the nephrons
3.26 Abnormalities of sodium and potassium By the end of Phase II students should be able to: • initiate investigation of hypo and hyper natraemia and hypo and hyper kalaemia • initiate management of these conditions