Download
1 / 27
270 likes | 359 Views
Medicare Savings Due to Prescription Drug Coverage for Near-poor Elders. Christine Bishop, Ph.D. 1 Andrew Ryan, M.A. 1 Daniel Gilden, M.S. 2 Cindy Parks Thomas, Ph.D. 1 Joanna Kubisiak, M.S. 2 Donald Shepard, Ph.D. (PI) 1 AcademyHealth Annual Research Meeting Washington June 8, 2008

E N D
Medicare Savings Due to Prescription Drug Coverage for Near-poor Elders Christine Bishop, Ph.D.1 Andrew Ryan, M.A.1 Daniel Gilden, M.S.2 Cindy Parks Thomas, Ph.D. 1 Joanna Kubisiak, M.S.2 Donald Shepard, Ph.D. (PI)1 AcademyHealth Annual Research Meeting Washington June 8, 2008 1Schneider Institutes for Health Policy, Heller School for Social Policy and Management, Brandeis University 2JEN Associates Inc.
Research Support Centers for Medicare & Medicaid Services CMS 500-00-0031/T.O. #2 Project Officers: William Clark and Karyn Anderson
Offset: Access to Prescription Drugs Expected to Reduce Use and Cost of other Health Services • Reduce or lessen acute illness episodes • Thus reduce health services use and cost (“offset effect”) • However, findings of previous research are mixed-e.g. • Significant or modest cost offsets: Shang (2005), Yang (2004) • No significant savings: Stuart (2004), Briesacher (2005) • Increased health services spending! Gilman (2004) • Studies of specific conditions are more likely to find offsets from providing Rx coverage See Cindy Parks Thomas, “How Prescription Drug Use Affects Health Utilization and Spending by Older Americans: A Review of the Literature“ http://assets.aarp.org/rgcenter/health/2008_04_rx.pdf
Study Question Is access to prescription drugs for near-poor elders associated with lower acute care utilization? • Hospitalization • Hospital days • Medicare spending
Prescription Drug Insurance Wisconsin SeniorCare Medicaid Waiver • Started September 2002 • Age 65+ • Income < 200% Federal Poverty Level (FPL) • Not Medicaid-eligible • No previous state drug plan for seniors • Enrollees unlikely to have had previous insurance (Waiver has been reauthorized through December 2009)
Wisconsin SeniorCare: Program Design • $30 enrollment fee • Deductible • 0 for enrollees with income less than 160% of FPL • $500 for income > 160% FPL • Copayments • $15 for brand-name drugs • $5 for generic drugs • No cap on benefits • Can enroll at any time
Coverage began September 1, 2002;Enrollment grew from 38,000 to 56,000 by December 2002
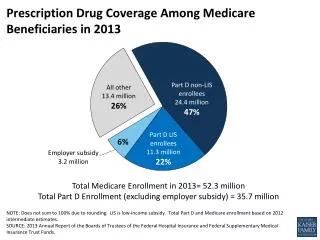
SeniorCare enrollees differ from aged Medicare populationBase Year Data (2001) Source: Medicare Enrollment Files 2001 All differences significant at p<.01
Enrollees: slightly more average monthly service use than all Medicare beneficiaries
Establish comparison group • Find Ohio elders who would have joined SeniorCare had it been offered to them • Age, sex, race, diagnoses • Medicare beneficiaries, not on Medicaid • Similar past health services utilization • Low income • Not insured for Rx drugs
Matched WI enrollees to comparison beneficiaries from Ohio • “Propensity score” (probability of enrollment) fitted on all WI beneficiaries with SSA income less than threshold – by SSA status group --all demographics plus • Health services use in 3 months prior to enrollment • Census block income distribution • SSA payments • For each WI enrollee -- locate OH beneficiaries with exact match on • 5-year age range, sex, race, urban-rural • Prior Medicaid eligibility, prior HMO enrollment • Nursing home status, index month • Social Security family status variables • From “exact match” group choose one with “nearest neighbor” propensity score
Time frame: Need full-year post-enrollment • Medicare data available through December 2003 only • Therefore include if enrolled through December 2002 • Enrolled in first 4 months • Outcome measures • Hospitalization- any admission • Hospital days • Total Medicare expenditures
Three Analytic Approaches • Compare means for post-index year • Relies on match and comparable prices, access • Compare differences in annual means, pre-post • Multivariate estimate of difference in differences for quarterly values
Hospitalization RatesWisconsin Enrollees and Ohio Matched Comparison N = 49,724*2 ***p < 0.01
Hospital DaysWisconsin Enrollees and Ohio Matched Comparisons N = 49,724*2 ***p < 0.01
Total Medicare ExpendituresWisconsin Enrollees and Ohio Matched ComparisonN = 49,034*2 ***p < 0.01
Difference in Difference Model Δ Outcomeit = β1Zi + β2 Δ Age squaredit + β3 Δ programit + β4 Δ programi,t-2 + β5Δprogrami,t-3 + β6 Δprogram i,t-4+ δΔquartert + εit Where Z is a vector of time invariant variables (gender, race, index age, income, diabetes, coronary heart disease, cerebrovascular disease, COPD, and arthritis) Program impact for period is computed as sum of coefficients β3 +β4 +β5 + β6
Wisconsin and Matched Ohio Comparison Difference In Difference Analysis (4 post-enrollment quarters) Robust standard errors in parentheses * p<.1 *** p<.001 Quarter Indicators and patient characteristics included
Limitations • Effects limited to first year • Long-term effects expected for pharmaceutical therapies • Have not yet fully accounted for selection into SeniorCare • First month enrollees were on wait list to join • Later month enrollees may have been impelled by new illness • State (OH vs. WI) health and regulatory systems differ • Could have affected both levels and differences • Matching limited to observed variables • Proxies only for low income status • Beneficiaries who died are included– answers program cost question, but needs more thought
Conclusions • Even in one year, near-poor enrollees in a pharmacy insurance program experienced reduced hospital use and Medicare savings • However, savings ($350 per year) are small relative to program cost (about $1030 per year) • Decline in services use suggests positive impact on health and wellbeing
Implications: Policy • For low-income seniors not previously covered by prescription drug insurance Medicare Part D coverage likely has a valuable health payoff • Savings in Medicare expenditures are unlikely to exceed program cost for beneficiaries in year one
Implications: Research • Impacts on health and services use over a longer time period may be larger • Extend studies to longer time frame • Advance matching methods: Use of income proxies is a contribution, but needs more work • SSA status • SSA payment amount • Census block distribution