Download

1 / 47
490 likes | 821 Views
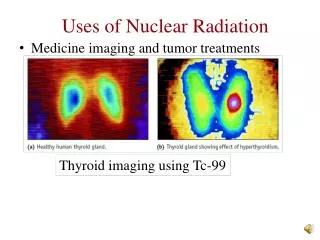
Tumor Imaging. We have a lot of selections for Tumor Imaging. Tumor is more metabolic active. 18F-FDG, 18F-FLT, 11C-acetate, 11C-cholin, 201Tl, 99mTc-MIBI. Tumor has specific receptors. 131I-MIBG, 131I-anti-AFP-MoAb Tumor can cause function and structure changes. BBB destruction, 99mTc-PMT

E N D
We have a lot of selections for Tumor Imaging • Tumor is more metabolic active. • 18F-FDG, 18F-FLT, 11C-acetate, 11C-cholin, 201Tl, 99mTc-MIBI. • Tumor has specific receptors. • 131I-MIBG, 131I-anti-AFP-MoAb • Tumor can cause function and structure changes. • BBB destruction, 99mTc-PMT • Tumor has specific gene expressions • antisense imaging
Objectives of This Part • FDG PET imaging • mechanism, imaging agent, image interpretation, clinical indications and usage. • 67Ga imaging • imaging agent, image interpretation, clinical indications and usage. Importance: ***, **, *
FDG PET imaging • Imaging agent: 18F-FDG • Imaging instrument: PET/CT or PET • Imaging procedure: • starvation for over 6h • 18F-FDG injection • wait 40-50 min • acquisition on PET/CT • image reconstruction
Molecular Mechanism Tumor Cell Vascular Glycogen 18FDG-1-P Hexokinase K1 18FDG-6- phospho- glucono-lactone K3 18FDG 18FDG 18FDG-6P HMP shunt K4 K2 Glucose-6- phosphatase 18F-fru-6-P Glucose transporter protein Glycolysis
Quantitative Parameters of PET-FDG Response • Standardized uptake value (SUV) • Uptake in tumor, normalized for dose injected and weight of the patient • Obtained as primary response parameter on every lesion (decay corrected dose/cc of tumor) SUV = (injected dose/patient weight (g))
Clinical Indications • Early detect and differentiate tumor. • Tumor staging and restaging. • Define tumor scope, especially for radiotherapy planning. • Therapy response monitoring. • Early differentiate regression or radiation necrosis. • Lead to correct treatment, save medical expenses.
FDG PET could detect tumors in their early stage and can be used for tumor screen
FDG PET can differentiate benign and malignant lesion more effectively.
Brain Tumor CP 696483High Grade recurrence post RT PET FDG TRANSAXIAL T-1 POST Gd 5 Oct 2000
Lymph node metastasis of lung carcinoma,CT is negative,but is positive in PET
FDG PET can monitoring early therapeutic response and predict outcome.
after chemo Before Chemo SUV=4.6
produced by cyclotron. • The half life of gallium-67 is 78 hours. • decays by electron capture.
Physiology Ga-67 acts as an iron analogue. Initially it binds to transferrin. The complex diffuses through loose endothelial junctions of capillaries at sites of inflammation and enters the extracellular fluid. Leukocytes migrate to sites of inflammation and degranulate, releasing large quantities of lactoferrin. Ga-67 has higher affinity for lactoferrin than transferrin. Ga-67 also attaches to siderophores of bacteria. Therefore can be used in leukopenic patients with bacterial infection and in detecting sterile abscesses that provoke a leukocyte response.
Areas where Ga-67 normally localizes • liver (site of highest uptake) • bone marrow • spleen • salivary glands • nasopharynx • lacrimal glands • breast uptake (especially in pregnant and lactating women) • kidneys and bladder in the first 24 hours - faint uptake can still be normal for up to 72 hours • mild diffuse lung uptake at 24 hours or less
Technique Common injection doses range from 3-6 mCi. Imaging should not usually be sooner than 24 hours - high background at this time produces false negatives.
Common Indications of gallium-67 imaging (1) • Whole-body survey to localize source of fever in patients with Fever of Unknown Origin (FUO). • Detection of pulmonary and mediastinal inflammation/infection, especially in the immunocompromised patient. • Evaluation and follow-up of active lymphocytic or granulomatous inflammatory processes such as sarcoidosis or tuberculosis.
Common Indications of gallium-67 imaging (2) • Diagnosing vertebral osteomyelitis and/or disk space infection where Ga-67 is preferred over labeled leukocytes. • Diagnosis and follow-up of medical treatment of retroperitoneal fibrosis. • Evaluation and follow-up of drug-induced pulmonary toxicity (e.g. Bleomycin, Amiodarone)
Gallium Tumor Imaging Gallium tumor localization is likely multifactoral, but in part related to leaky capillary membranes in tumors, and the presence of iron-binding proteins such as ferritin which are found in increased concentrations in tumors.
Bronchogenic carcinoma • Squamous cell carcinoma has the highest (gallium avidity). • adenocarcinoma has the lowest detection rate. • gallium has a overall sensitivity of about 90% for the detection of primary bronchogenic carcinoma. • Lesions smaller than 1.5 cm are difficult to detect. • Lack of gallium accumulation in a lesion is still associated with a 24% probability for malignancy.
Hodgkin's lymphoma • Overall sensitivity for detecting Hodgkins lymphoma is about 85%, with a specificity of 90%. • Gallium scintigraphy can also be used to predict patient response to treatment after initiation of chemotherapy.
nodal uptake of tracer in the neck and mediastinum in this patient with Hodgkins disease.
Non-Hodgkins Lymphoma • Gallium sensitivity is reported to be better than 85% for high grade tumors. • Sensitivity for low grade (slow growing) tumors is poor. • A persistently positive Ga-67 exam after one cycle of treatment or at midtreatment for non-Hodgkins lymphoma is associated with a higher likelihood for treatment failure, while a negative scan implies a favorable prognosis.