Download
1 / 39
390 likes | 411 Views
Learn about the sources and control of plasma glucose, hormonal regulation, clinical signs, diagnosis, and treatment of Diabetes Mellitus. Detailed insights into insulin, glucagon, glucose metabolism, and complications.

E N D
Endocrine Diseases Dr/Abd Elghany Hefnawy
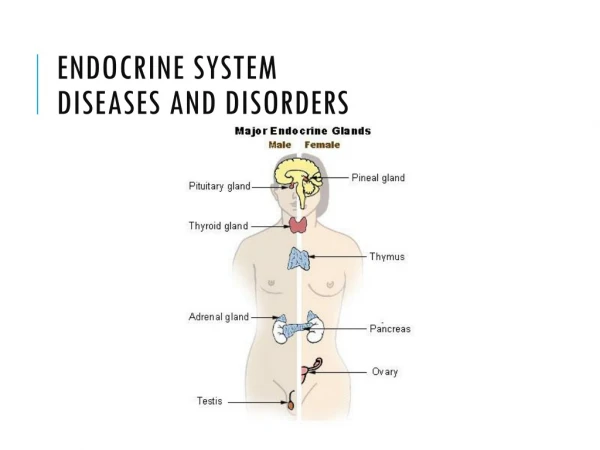
Anterior Posterior PAO PTH Adrenalin,Noradrenalin Corticosteriods T3&T4 Insulin Glucagon
Diabetes Mellitus (DM) Dr/Abd Elghany Hefnawy
Sources & control of plasma glucose
Sources Fat Glycerol Glycogen Gluconeogenesis Alanin (AA) Glycogen Glycogenolysis Glucose Intestine
Control Hormonal control of blood glucose Promotes glycogenesis (formation of glycogen) Insulin (Beta cells) Activation of Acetyl carboxylase enzyme Essential for FFA (Free fatty acids) Triglycerides + Fat (Lipogenesis)
Insulin Activation of hexokinase enzyme Essential for Phosphorylation Essential for Glucose entrance and metabolism inside the cells
Glucagon (A cells) Stimulates the process of glycogenolysis for formation of glucose Promotes the mobilization of the hepatic storage of glucose to the blood (i.e it has hyperglycemic action)
Brain tissue is very sensitive to low glucose level causing secretion of ACTH Growth Hormone Cortisol Lipolysis Increase mobilization of amino acids From the muscles to be converted into Glucose in the liver (Gluconeogenesis) Antagonism of Insulin actions
Lipolysis Production of keton bodies Acetone Adour of the breath (Ketoacidotic stage)
Definition It is a chronic complex disorder of carbohydrates, lipid and protein metabolism as a result of Inability to produce or utilization of an adequate amount of insulin.
Etiology Damage or destruction of pancreatic β-cells due to Trauma or neoplasm Pancreatitis Hereditary Depletion or aplasia Of β-cells (Idiopathic) (I) Insulin dependent DM
Overeating causing obesity Excess of growth hormone Excess of Glucagon hormone Excess of Glucocorticoides or cortisol therapy Hyperthyroidism (II) Insulin independent DM
Predisposing factors Sex (more in females) Old age (8 years) Adrenalin and nor adrenalin Obese animal
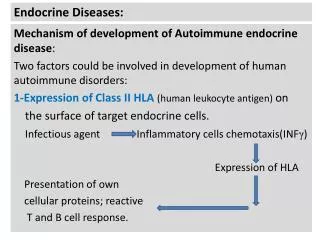
Etiology and predisposing factors Pathogenesis Clinical findings
Etiology and predisposing factors Disturbances of entrance of glucose intracellular Low insulin level Hyperglycemia DM
When Glucose level more than 180-220 mg/dl Kidney cannot reabsorb glucose Loss of glucose (Energy) Glucosueria Glucose in urine increases the osmotic pressure Dehydration and Thirst Polyueria
Polyphagia Loss of glucose (Energy) Glucosueria Dehydration and Thirst Polyueria Polydepsia
Polyueria Polyphagia Polydepsia Thirst Dehydration Weakness and emaciation
Vomiting Neuropathy Corneal opacity
Renal failure Coma & Death Emaciation
Diagnosis Case history (Etiology and predisposing factors) Clinical signs Laboratory diagnosis
Laboratory diagnosis Glucose GTT (Glucose Tolerant Test) Blood glucose Urine glucose (Glucoseueria) Fasting (60-100 mg/dl) Random (up to 150 mg/dl) When Blood glucose more 180-220 mg/dl
GTT (Glucose Tolerant Test)
Laboratory diagnosis High Keton bodies High GOT GPT Lipase & Amylase High urine Sp Gravity (N= 1.025) Low Insulin
Mild Moderate Sever Dangerous Restricted Feeding System 80% protein 20% carbohydrate Mild + Oral insulin Or Hypoglycemic drug as chloropamide Mild + S/C Insulin 2IU/Kg Sever + Fluid therapy
وسائل التواصل Email: abdelghani72@yahoo.com Abdelghany.hefnawy@bu.edu.eg Facebookabdelghanyhefnawy د.عبد الغني حفناوي Web site to download lectures www.bu.edu.eg/staff/abdelghanyhefnawy (Courses) Tel 01011676482