Download
1 / 49
610 likes | 2.24k Views
PITUITARY GLAND. Where is it located??? Name its’ 3 parts or sections. What hormones are secreted by the pituitary gland???. Pituitary Gland. ANTERIOR PITUITARY. SECRETES 6+ HORMONES: ACTH (adrenocorticotropic hormone) release of cortisol in adrenal glands

E N D
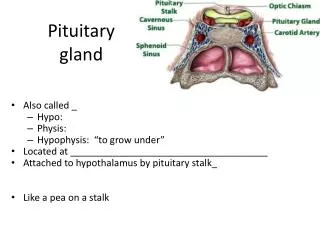
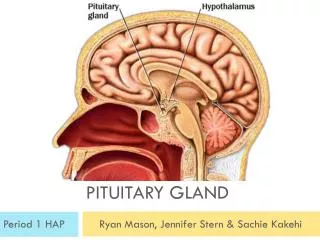
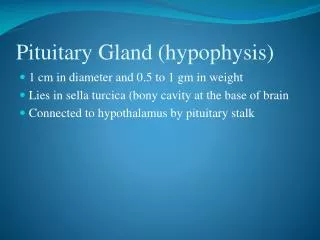
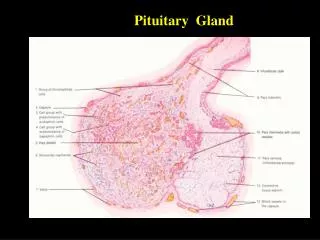
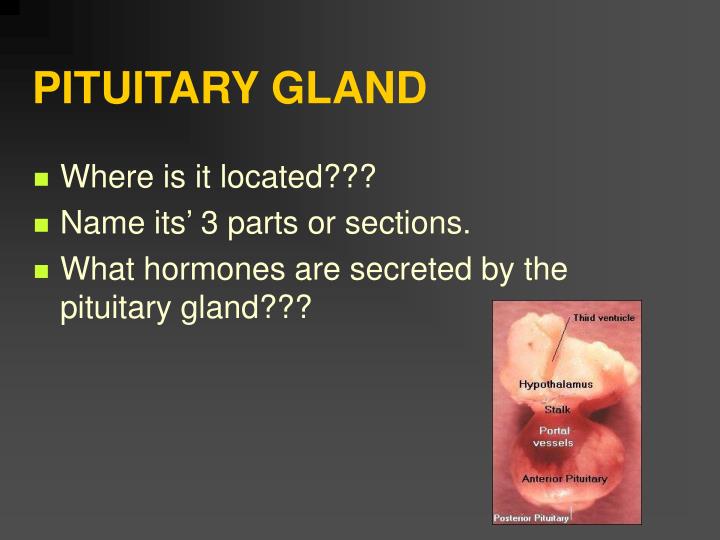
PITUITARY GLAND • Where is it located??? • Name its’ 3 parts or sections. • What hormones are secreted by the pituitary gland???
ANTERIOR PITUITARY • SECRETES 6+ HORMONES: • ACTH (adrenocorticotropic hormone) release of cortisol in adrenal glands • TSH (thyroid stimulating hormone) release of T3 & T4 in thyroid gland • GH (growth hormone) stimulates growth of bone/tissue
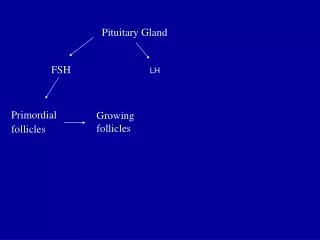
FSH (follicle stimulating hormone) stimulates growth of ovarian follicles & spermatogenesis in males • LH (lutenizing hormone) • regulates growth of gonads & reproductive activities • Prolactin promotes mammary gland growth and milk secretion
ANTERIOR HYPER PITUITARY DISORDERS • What would happen if you had TOO MUCH secretion of prolactin? • Too much release of Lutenizing Hormone (LH)?
ANTERIOR HYPER PITUITARY DISORDERS • ETIOLOGY • Primary: the defect is in the gland itself which releases that particular hormone that is too much or too little. • Secondary: defect is somewhere outside of gland i.e. GHRH from hypothalamus TRH from hypothalamus
PITUITARY TUMORS • 10% OF ALL BRAIN TUMORS • What are the diagnostic tests to diagnose a pituitary tumor? • tumors usually cause hyper release of hormones
ANTERIOR PITUITARY-HYPERfunctioning Sing along • What would happen if you had too much growth hormone secretion??? • Which goolish character on the Addam’s Family may have had too much GH secretion?
TOO MUCH GROWTH HORMONE • GIGANTISM IN CHILDREN • skeletal growth; may grow up to 8 ft. tall and > 300 lbs • ACROMEGALY IN ADULTS • enlarged feet/hands, thickening of bones, prognathism, diabetes, HTN , wt. gain, H/A, • Visual disturbances, diabetes mellitus
GIGANTISM IN CHILDREN • ACROMEGALY IN ADULTS
MEDICAL INTERVENTIONS FOR PITUITARY TUMOR • Medications • Parlodel (bromocriptine) to ________ & GH levels. • Radiation therapy • external radiation will bring down GH levels 80% of time
Neurosurgery: • procedure called “transsphenoidal hypophysectomy”; New Method • Most common method: incision is made thru floor of nose into the sella turcica.
Nursing Management • Pre op hypophysectomy • Anxiety r/t • a. body changes • b. fear of unknown • c. brain involvement • d. chronic condition with life long care • Sharmyn
Sensory-perceptual alteration r/t a. visual field cuts b. diplopia • secondary to pressure on optic nerve. • Alteration in comfort (headache) r/t a. tumor growth/edema
Knowledge deficit r/t • Post-op teaching • pain control • ambulation • hormone replacement • activity
Post operative care • Post-op complications of hormone insufficiency: • What would happen if you didn’t have enough ADH? • What is that disorder called?
Other insuffciency: • Decrease ACTH will require cortisone replacement due to decrease glucocorticoid production. • Can you live without glucocorticoids????
Other deficiency: • in sex hormones can lead to infertility due to decrease production of ova & sperm • What were those hormones called again?-
Incisional disruption after transsphenoidal hypophysectomy • Avoid bending and straining X 2 months post transsphenoidal hypophysectomy, • Use stool softeners • Avoid coughing • Saline mouth rinses • No toothbrushes for 7-10 days
Post-op CSF Leak where sella turcica was entered • any clear rhinorrhea - test for glucose • + glucose = CSF Leak • Notify physician • HOB 30 degrees • Bedrest
CSF leak usually resolves within 72 hrs. • If not - spinal taps done to decrease pressure
Post op problems cont. • Periocular edema/ecchymosis • Headaches • Visual field cuts/diplopia • What is the most important nursing intervention for these problems????
ANTERIOR PITUITARY-Hypofunction • 1. Etiology (rare disorder) may be due to disease, tumor, or destruction of the gland. • Diagnostic tests • CT Scan • Serum hormone levels
S & S Anterior Pituitary Hypofunctioning • GH • FSH/LH • Prolactin • ACTH • TSH
Medical Management • neurosurgery -- removal of tumor • radiation - tumor size • hormone replacement • cortisol, thyroid, sex hormones
Nursing Management • Assessment of S & S of hypo or hyper functioning hormone levels • Teaching-Compliance with hormone replacement therapy • Counseling and referrals • Support medical interventions
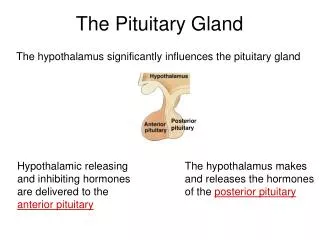
Posterior Pituitary(Neurohypophysis) Question??? What hormones are released by the posterior pituitary? _____ & _____are released when signaled by hypothalamus
ADH (Vasopressin) • secreted by cells in the hypothalmus and stored in posterior pituitary • acts on distal & collecting tubules of the kidneys making more permeable to H20 -- or volume excreted?
Bonus Round... • Under what conditions is ADH released??? • ADH has vasoconstrictive or vasodilation action???
ANSWERS: • released in response to decrease blood volume, increase concentration of Na+ or other substances, pain, stress • ADH has vasocontrictive properties
Oxytocin • Controls lactation & stimulates uterine contractions • ‘Cuddle hormone’Research links oxytocin and socio-sexual behaviors
Posterior Hyper pituitary Disorders • SIADH (TOO MUCH ADH!!) • lung cancer, Ca duodenum/pancreas, trauma, pulmonary disease, CNS disorders, drugs -- Vincristine, nicotine, general anesthetics, tricyclic antidepressants
Think tank: • If you are having too much ADH... What would the clinical signs/symptoms be??
Clinical manifestations-SIADH • Weight gain or weight loss? • or urine output? • or serum Na levels? • weakness • muscle cramps • H/A • Diarrhea
If hyponatremia worsens will develop neuro manifestations • lethargy • decrease tendon reflexes • seizures
Diagnostic Tests-SIADH • Serum Na+ <135meq/l • Serum osmolality <275 OSM/kg H2O • urine specific gravity • or normal BUN
Medical Treatment • ***FLUID RESTRICTION • LIMIT TO 1000ML/24HRS • IV 3% NaCl to replace Na • IF CHF -- Lasix (temporary fix) • Treat underlying problem --Chemo, radiation • Declomycin 600 po-1200mg/day to inhibit ADH
Nursing Interventions-SIADH • Fluid restriction may be as little as 500-600ml/24hrs • Daily weights... • 1 lb. weight = 500ml fluid retention • Accurate I & Os
Nursing Management-SIADH • F & E imbalances • fluid intake • High risk for injury r/t complications of fluid overload (seizures)
Posterior HypopituitaryADH disorders Diabetes Insipidus (too little ADH) What do you think the S&S would be if you had too little ADH???
Etiology • 50% idiopathic • a. central -- i.e. brain tumors • b. nephrogenic - inability of tubules to respond to ADH
Clinical Manifestations-DI • Polydipsia • Polyuria (10L in 24 hours) • Severe fluid volume deficit • wt loss • tachycardia • constipation • shock
Diagnostic Tests-DI • or urine specific gravity orserum Na orserum osmolality • Dehydration test: • 2 units of Vasopressin (ADH) mixed in saline administered over 2 hrs then check urine osmolality levels
Medical Management-DI • Identification of etiology, H & P • Tx of underlying problem • DDAVP (nasal spray) • Pitressin s.c. IM, nasal spray
Nursing Management-DI • Assess for F & E imbalances • High risk for sleep disturbances • Increase po/IV fluids • RF Injury (hypovolemic shock) • Knowledge deficit • High risk for ineffective coping