Download
1 / 68
700 likes | 911 Views
Safe & Effective Handoffs Subha Airan-Javia Penn Hospitalist Medicine. It happened at a hospital you know…. 9am rounds : 70 yo woman with DVT & h/o GI bleed On heparin with 48 hours of very elevated ptts (>150) Altered mental status & low BP CBC ordered 1pm postcall signout : “ f/u CBC ”

E N D
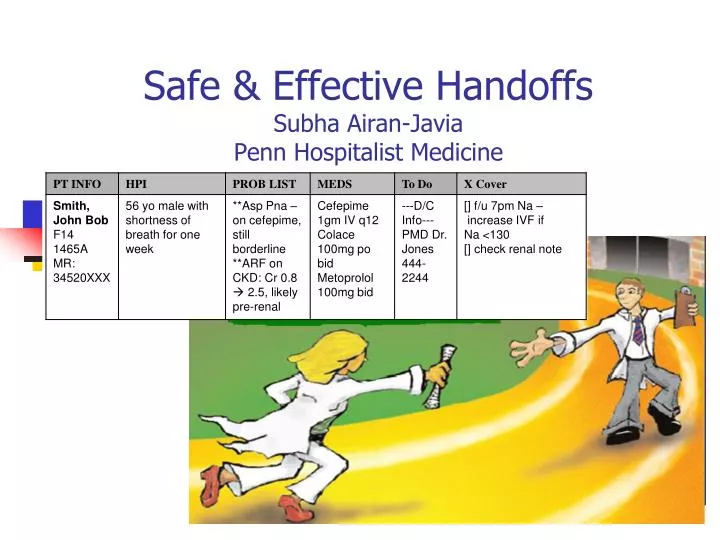
Safe & Effective HandoffsSubha Airan-JaviaPenn Hospitalist Medicine
It happened at a hospital you know… • 9am rounds:70 yo woman with DVT & h/o GI bleed • On heparin with 48 hours of very elevated ptts (>150) • Altered mental status & low BP CBC ordered • 1pm postcall signout:“f/u CBC” • No mention of elevated PTTs or concern for GI Bleed as potential cause of altered mental status and low BP • 3pm: Hgb = 4.0 • Wasn’t believed, another hgb was sent, no transfusion • 5pm: Patient had melena, hypotension, transferred to the ICU. • Repeat CBC confirmedHgb of 4. • Patient quickly coded and expired in ICU
Think About it… • Did a poor handoff contribute to this patient outcome? • Did this patients get the care that she expected from our hospital? How about the care that you and I expected?
Fear of making a mistake and harming a patient • Natural fear • You will make errors; we all do • Did parts of the hospital system make the error easy to happen? • If so, someone else needs to know (chief resident, program meeting, incident reporting system) • Take care of yourself and each other
Goals for Today • Get you ready to perform safe handoffs! • Review the importance of handoffs • Teach the components of a good electronic and verbal handoff • Practice handoffs in a simulated environment
Facts • Discontinuity in the hospital is inevitable • Discontinuity is increasing in teaching hospitals due to duty hour regulations • Lack of communication is the most common root cause of medical errors nationally • Communication breakdowns during handoffs can have deleterious effects on our patients
More Facts… • Improving Handoffs is a National Patient Safety Goal (NPSG 2E) • Implement a standardized approach to “handoff” communications including an opportunity to ask and respond to questions
Being Covered by a cross-cover resident is a powerful risk factor for preventable adverse events. Petersen, L. A. et. al. Ann Intern Med 1994;121:866-872
Bringing it closer to home… 6 Residents, 7 Handoffs in 5 days Day 1 ED Resident Nightfloat JAR Intern A - Shortcall Day 2 On Call Intern #1 Intern A Day 3 On Call Intern #2 Intern A (now on Call) Day 4 Dayfloat Day 5
Even more handoffs in the ICUs… ED Resident Day 1 Primary On-Call team Dayfloat Day 2 Nightfloat Nightfloat Day 3 Primary Team 4-5 Residents, 5 Handoffs in 48 hours
A handoff example…. Location: Founders 14 nurses station Time of Day: 12:30pm post-call People: Two July interns who don’t really know each other yet.
What did you notice? • Noisy environment • Multiple interruptions • Delivery is not standardized • No time for questions, reiteration of plan
Verbal Handoff Tips • Location: as quiet as possible (away from the nursing station, not in the ED) • Minimize interruptions • Start patient over if unavoidable • If you are worried about the patient…say it first! • Give on-call intern an opportunity to ask questions and repeat back important facts • Review every patient • Follow the same format/order for all patients
Verbal Handoff Format • PROBLEM BASED • Sick/Not Sick • Code status (if not full code) • 1-3 sentences history • PROBLEM LIST • Active issues for each • Relevant Data and Meds • Crosscover list • If/then statements, anticipatory guidance
Electronic Handoff: Purpose • Reference for primary team • Reference for covering provider Repository of information Discharge summary A Novel
Electronic handoff plan • Problem list owned by Interns • Rest of handoff primarily resident responsibility July – Jan • Interns should participate, edit what they can handle • Increase your share of handoff involvement
Handoff Progress Note • Problem List • 50 Thousand foot view of problems with short assessment & overall plan • Important medications & radiology associated with problems • Antimicrobials, anticoagulation, immunosuppressants, Narcotics • Concise, bulleted
Electronic Handoff Tips • Standardize: Keep info in designated location • Exclude/Remove irrelevant information • Clean-up and update handoff regularly • Avoid non-standard abbreviations • MS: multiple sclerosis, mental status, or morphine sulfate? • HL: Hyperlipidemia or Hodgkin’s Lymphoma? • Summarize findings. Do not cut and paste results
Electronic Handoff Tips • Problem list should be complete, but concise • Should not be your entire progress note word for word • This is the basis of your verbal handoff • Should be updated & reprioritized as new problems arise and old ones change
And don’t forget… • The sign-out is a TEAM document • Read by ALL disciplines in the hospital • Unprofessional language and statements should never be written
Keys to a Good Handoff The Nitty Gritty
Approach to verbal handoff Sick not sick History, Hospital Course Objective data Upcoming plan, dispo To do
Approach to verbal handoff [H O U] S T
Approach to verbal handoff S = SICK/NOT SICK 30 seconds -Name -Code Status -Culture/Family etc
Approach to verbal handoff H = History 1-2 sentences (1 minute) What brought the patient to the hospital Similar to your ASSESSMENT statement on your A/P
Approach to verbal handoff “H O U” Active Problems, Hospital course, Objective data & Plan for each MAIN AREA OF FOCUS
Approach to verbal handoff T = To Do SECOND AREA OF FOCUS -Go through each cross cover to do item, what needs to be done, rationale & action plan -If/Then statements or other guidance
Patient Information Automatically imported from SCM
Start with name & status: If you are worried about the patient, say it now - up front. Write it in the crosscover section. “John Smith is very sick” ; “I’m worried about Mrs Jones” Code Status: If not Full Code, always state this verbally. “He is DNR A” Access, Culture Limits, Precautions: mention if relevant Contact information: Emergency contact for patient. “This family wants to be called with every change or new problem, even if in the middle of the night”; “No contact person has been located yet for this patient with dementia” Patient Information
History & Relevant Data Automatically imported from SCM
History: State the chief complaint at first – once you know the diagnosis, you should UPDATE it. Short history. Admission vitals if they are relevant. “45 y/o female with abdominal pain” “89 y/o male with pneumonia.” Important Hospital Events: Mention things that could come up overnight “Desatted last night and responded to IV lasix” Data and Micro: Summarize findings, do not cut and paste results!! History & Relevant Data
History & Relevant Data Too Wordy… MUCH BETTER!
List all Active Problems: Include salient points of plan and important results. “For aspiration pna – patient is on cefepime, 10 day course. He also has renal failure & hyponatremia – likely because of dehydration. Diarrhea is concerning for CDiff” Problem List Document Relevant Physical Exam Findings: “Mr S. has dementia but is able to converse well and can tell you if he is in pain” “Mr J has CHF, her lungs always have rales..” Chronic Problems: place chronic or inactive problems at the bottom of the list
Info is nice to have, but too much! Makes the prob list too long to sort through in a rush Summarize study in the Data section. Put relevance for day to day care here
Problem List • Mention things that on-call interns have been called about every night • “This patient sundowns every evening…and here is the plan should it happen tonight…” • Review important exam findings and always think about including mental status • “Mrs. J has severe asthma flare, lung exam is severe wheezing and little air movement on exam today” • “Mr S.has dementia and only oriented x 1, but always able to follow commands, tell you if he’s in pain, etc”
Medications Automatically imported from SCM
Important Meds Should Be Verbally Reviewed & Highlighted: Antimicrobials, Anticoagulants, Narcotics, Benzos “For pneumonia, patient is on cefepime, plus flagyl for possible CDiff, and warfarin for a low EF.” Medications • Mention any important changes in meds: New meds, Discontinued meds, Dose Changes “For HTN he is on metoprolol, but we had to decrease his dose today because of bradycardia. So if he is hypertensive, I would use something else.”
Medications Other med info: Medications dosed by level, ordered daily, recent antibiotics, abnormal reactions For warfarin, use “warfarin dose daily” order
D/C Info – Outpatient MD information, appointments to be made after discharge, any discharge related item To Do – Items for the primary team to do (today or later in the admission) Crosscover teams will look at this too D/C Info & To Do List