Download
1 / 12
120 likes | 235 Views
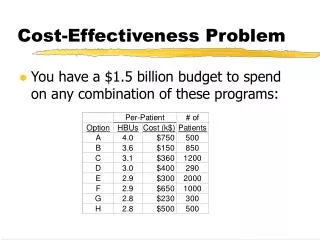
Cost-effectiveness of harm r eduction. David P Wilson. Why worry?. UNAIDS, 2012. What HR interventions work?. Three proven priority interventions NSP OST ART

E N D
Cost-effectiveness of harm reduction David P Wilson
Why worry? UNAIDS, 2012
What HR interventions work? • Three proven priority interventions • NSP • OST • ART • 9-component comprehensive package, endorsed by WHO, UNODC and UNAIDS - Three priority interventions plus HCT, condoms, IEC, STI, HCV and TB prevention/treatment
What we know about NSPs • Review of evidence from 42 studies (Gibson et al, 2001) • 28 showed a favorable outcome • 2 showed an unfavorable outcome • Others showed no clear results or mixed findings • Ecological studies: 81 cities (Hurley et al, 1997)
What we know about NSPs • Led to incidence declines • E.g. New York City: 4% to 1% • Many places without NSPs have had large increases • E.g. Sargodha, Bangkok, Manipur, Cebu • Reasons are obvious • Behavior in British Columbia exemplifies (Vancouver, Victoria)
What are the cost ranges?NSPs • Average cost of NSP provision $23–71 /year 1 • NSP cost varies by region and delivery system 2 1 UNAIDS 2007 resource estimations; Schwartlaender et al 2011. 2 UNSW estimates, based on 10 studies identified in the 6 regions
Cost-effectiveness of NSPs • Systematic review (Jones 2006) • 13 economic studies [most in North America]: all concluded that NSPs were cost-effective or cost-saving compared to lifetime cost of HIV • Net financial benefits of NSPs in all regions; both high- and low- income settings • E.g. China (Ni et al 2012) • USA (Hrishikesh et al 2008) • Bangladesh (Guinness et al 2008) • Australia (Kwon et al 2012)
What we know about OST • All randomized controlled trials of OST have produced positive results (Mattick et al, 2003) • OST reduces injecting activity (Cochrane Syst. Review; Gowing, 2008; Mattick, 2009) • Meta-analysis (North America, Europe & Asia) • 54% reduction in HIV acquisition
What we know about OST and the importance of combining the priority HR interventions to achieve impact Empirical evidence: NSP + OST at scale: Amsterdam cohort study - 57% HIV incidence reduction, 64% HCV incidence reduction (incidence reductions low if service uptake partial). Similar findings in Central Asia. Source: Van Den Berg et al, 2008
What are the cost ranges?OST 2 1 UNAIDS 2007 resource estimations; Schwartlaender et al 2011. 2 UNSW estimates, based on 10 studies identified in the 6 regions • Average OST cost : Methadone 80 mg: $363 - 1,057 / year; Buprenorphine, low dose: $1,236 – 3,167 /year1 • OST consistently far costlier than NSP
Priority HR intervention packages are cost-effective and cost-saving • Estimated cost-effectiveness ratios for priority intervention package favorable in all regions • costs per HIV infection averted: $100 to $1,000 • In all regions with data on return on investment, harm reduction packages are cost-saving • Total future ROI $1.1 – 8.0 (3% discounting)
Conclusions • Globally, harm reduction interventions are good value for money, improving health outcomes for PWID. • ~US$100 to $1,000 per HIV infection averted • NSPs: Moderate-to-strong effectiveness and cost-effectiveness or even cost saving! • OST: Strong evidence for effectiveness. • Questionable cost-effectiveness when considering just HIV or HCV alone; moderate cost-effectiveness when drug-related issues included • OST + NSP: Strong cost-effectiveness • ART: Cost-effective for survival, weak evidence for prevention, PrEP not cost-effective