Download

1 / 19
• 200 likes • 303 Views
Cost effectiveness of Isoniazid profylaxsis. Children with HIV in South Africa. Background. Isoniazid is a drug against tubercholosis Tubercholosis and HIV are dual pandemics in sub saharan Africa 1 Tubercholosis accellerates the course of HIV 1

E N D
Cost effectiveness of Isoniazid profylaxsis Children with HIV in South Africa
Background • Isoniazid is a drug against tubercholosis • Tubercholosis and HIV are dual pandemics in sub saharan Africa1 • Tubercholosis accellerates the course of HIV1 • HIV increases tubercholosis incidence by reactivation of latent infection and rapid progression of recent infections2. • Studies has shown different results of the cost effectiveness of Isiniazid3.
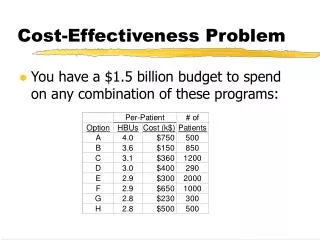
Intervention1 • To centered randomized controlled • South Africa, Cape Town • 29.5 % of South Africas population infected with HIV (2004) 2 • Tuberculosis incidence in South Africa is 599/100.000 (2005) 2 • Children with HIV, median age 24 months • Placebo and Isoniazid was given with Co-trimoxazole (antibacteriael)
Intervention1 II • 277 randomised - 14 exclude = 263 • 9 % received HAART (highly active antiretroviral treatment) • Three days a week or every day • January 2003 to 17 May 2004 (ended because of results). Estimated average days = 486 (1,33 years / 16 months)
Effects of intervention I * Estimation Note: The mechanism for reducing mortality is unclear
Model: Decision tree I Start of study: 0 months End of study: 16 months Time γ Dead: 8.33 % Dead: w Alive : 91.67 % Isoniazid Alive: Y Dead: 16.03 % Placebo Dead: w Alive: 83.97 % Alive: y
Assumptions calculating effects of intervention, model I • Average age at initiation: 24 months (=median)* • Average age at death in intervention: 32 months** • Average life expectancy at end of intervention when “alive”: 33 months*** * Estimation: median age ** Estimation: half way of study *** Estimation based on 365 – 730 day survival probability interval in 5 (mortality ratio = 0.0005 * days).
Model: Decision tree II Start of study: 0 months End of study: 16 months Time γ Dead: 8.33 % Dead: W Tuberculosis: X Tuberculosis: 3.79 % Dead: Y Isoniazid Tuberculosis: Z ”Well”: 87.88 % ”Well”: Æ Dead: 16.03 % Dead: W Placebo Tuberculosis: X Tuberculosis: 9.92 % Dead: Y Tuberculosis: Z ”Well”: 74.05 % Alive: Æ
Assumed time line Avr. time for death after study: 73 m. Study starts: 24 m. End of study: 40 m. Avr. time for death in study: 32 m. Death w. "well" after study: 74 m. Death w. TB after study: 56 m. Birth: 0 m.
Assumptions calculating effects of intervention, model II • Average age at initiation: 24 months* • Average age at death in intervention: 32 months** • Average life expectancy at end of intervention when “well” or “tuberculosis”: 33 months*** • Average life expectancy at end of intervention when “Tuberculosis”: 17 months**** • Average life expectancy at end of intervention when “well”: 34 months***** * Estimation: median age ** Estimation: half way of study *** Estimation based on 365 – 730 day survival probability interval in 5 (mortality ratio = 0.0005 * days). *** Estimated as half of average **** Estimated as residual to "tuberculosis"-group
Costs4 • South Africa, Cape Town (2001-2002) • Adjusted 3 % p.a. to 2009-prices Incremental costs to co-trimoxazole Drug cost • Cost of 12 months of IPT: $ 22 • Cost of 16 months of IPT: $ 29 Drug and screening cost • Cost of 16 months of IPT and screening of participants: $ 81 • Cost of 16 months of IPT and screening: $ 120
Cost effectiveness Model I • Cost per person: $ 29 • Effect per person: 0,21 years • Incremental cost effectiveness ratio: $ 140 $ per life year Model II • Cost per person: $ 29 • Effect per person: 0,31 years • Incremental cost effectiveness ratio: $ 95 per life year
Conclusion • The incremental cost-effectiveness ratio was calculated to: $ 95 / 140 • Sensitivity analysis showed a variation from: $ 70 - 220 per life year • Well under threshold • The cost effectiveness ratio when including selection process was: $ 192 - 900 per life year • Prophylaxis with Isoniazid offers a cost effective public health intervention when it is directed to children with HIV in areas with a high incidence of tuberculosis • Especially when access to ART or HAART is limited
Discussion Results • Isoniazid is cost effective in this case - when you compare with western standards • However counseling and other no-drug prevention methods has been shown to be far more cost effective since HIV-infections are averted(see 4). • Can you compare the two sets of interventions? Analysis • Lack of data makes it difficult to live up to high standards of economic evaluation(see 6). • Especially data for mortality / life expectancy for children with HIV was inaccurate(for variation see 5,7,8).
References 1: Zar HJ, Cotton MF, Strauss S, Karpakis J, Hussey G, Schaaf HS, Rabie H, Lombard CJ.: Effect of isoniazid prophylaxis on mortality and incidence of tuberculosis in children with HIV: randomised controlled trial. BMJ. 2007 Jan 20;334(7585):105-6. 2: Hausler HP, Sinanovic E, Kumaranayake L, Naidoo P, Schoeman H, Karpakis B, Godfrey-Faussett P: Costs of measures to control tuberculosis/HIV in public primary care facilities in Cape Town, South Africa. Bull World Health Organ. 2006 Jul;84(7):528-36. 3: Holland DP, Sanders GD, Hamilton CD, Stout JE. Costs and cost-effectiveness of four treatment regimens for latent tuberculosis infection. Am J Respir Crit Care Med. 2009 Jun 1;179(11):1055-60. Epub 2009 Mar 19. 4: Hogan DR, Baltussen R, Hayashi C, Lauer JA, Salomon JA. Cost effectiveness analysis of strategies to combat HIV/AIDS in developing countries. BMJ. 2005 Dec 17;331(7530):1431-7. Epub 2005 Nov 10. 5: Newell, Marie-Louise; Coovadia, Hoosen; Cortina-Borja, Marjo; Rollins, Nigel; Gaillard, Philippe; Dabis, Francois. Mortality of infected and uninfected infants born to HIV-infected mothers in Africa: a pooled analysis. Lancet, 10/2/2004, Vol. 364 Issue 9441, p1236-1243, 8p; 6: Drummond, MF, Schulper, MJ, Torrance, GW, O'Brien, BJ, Stoddart, GL. Methods for the Economic Evaluation of Health Care Programmes. 2005: Third edition, Oxford: Oxford University Press. 7: de Martino M, Tovo PA, Balducci M, Galli L, Gabiano C, Rezza G, Pezzotti P. Reduction in mortality with availability of antiretroviral therapy for children with perinatal HIV-1 infection. Italian Register for HIV Infection in Children and the Italian National AIDS Registry.JAMA. 2000 Jul 12;284(2):190-7. 8: Taha E. Taha, Stephen M. GrahamDagger, Newton I. Kumwenda, Robin L. Broadhead, Donald R. Hoover, Diane Markakis, Len van der Hoeven, George N. Liomba, John D. Chiphang, Paolo G. Miotti. Morbidity Among Human Immunodeficiency Virus-1-Infected and -Uninfected African Children.PEDIATRICS Vol. 106 No. 6 December 2000, p. e77.