Download
1 / 43
430 likes | 1.16k Views
ACUTE RHEUMATIC FEVER IN INDIA. – A MYTH OR A REALITY AT PRESENT. Rheumatic fever - 2010. An immunologically mediated Connective tissue disease Consequence of throat infections With group A Streptococci involving joints, (transient) heart and to lesser extent central nervous system.

E N D
ACUTE RHEUMATIC FEVER IN INDIA –A MYTH OR A REALITY AT PRESENT Rheumatic fever - 2010
An immunologically mediated • Connective tissue disease • Consequence of throat infections • With group A Streptococci involving joints, (transient) heart and to lesser extent central nervous system. • Tonsillopharynx region
EPIDEMIOLOGY • The prevalence of acute rheumatic fever was 0.05 to 1.7/ 1000 from 1940 to 1983 and 0.18 to 3/1000 from 1984-1995 and much lower in the last decade. • The average age of presentation had been reported by Dr. Padmavathi to be between 10 to 14 years.
The decline in incidence of Acute rheumatic fever in the last decade can be attributed to • Improved socio-economic status of the community • Diminished streptococcal virulence! • Presence of fewer Rheumatogenic serotypes
Rheumatic fever is a systemic disease affecting the peri-arteriolar connective tissue
Immunological cross reactivity between streptococcal antigen and host antigens due to “molecular mimicry”. • It is Type II hypersensitivity reaction.
Tonsillopharyngeal infection, no other sites Intensity of the infection Brisk antibody response Persistence of the organism Rheumatogenic strains M types 1, 3, 5, 6, 14, 18, 19, 27 and 29 Distinct structural characteristics of M proteins Long terminal antigenic domain Epitopes shared with human heart tissue Heavily encapsulated, forming mucoid colonies Does not produce opacity factor SUSCEPTIBLE HOST Genetic predisposition Presence of specific B-cell alloantigen High incidence of class II HLA antigens
Cell wall "M proteins" which are highly antigenic. • The antibodies against the "M proteins" may cross react with cardiac myofiber protein myosin, heart muscle glycogen and smooth muscle cells of arteries. • Histologically characteristic Aschoff bodies, composed of swollen eosinophilic collagen surrounded by lymphocytes and macrophages can be seen on light microscopy.
Aschoff’s nodes pathognomonic granulomatous lesion Present in stromal connective tissue of the myocardium around blood vessel
Central fibrinoid material • Surrounded by histiocytes • Lymphocytes, plasma and giant cells • The characteristic histiocyte or Anitschkow, cells are large with a slightly basophilic cytoplasm • The nuclei may resemble ‘owls’ eyes’
serofibrinous Pericardial exudates
fibrinoid necrosis and verrucae formation along the lines of closure of the left-sided heart valves, warty projections MacCallum plaques.
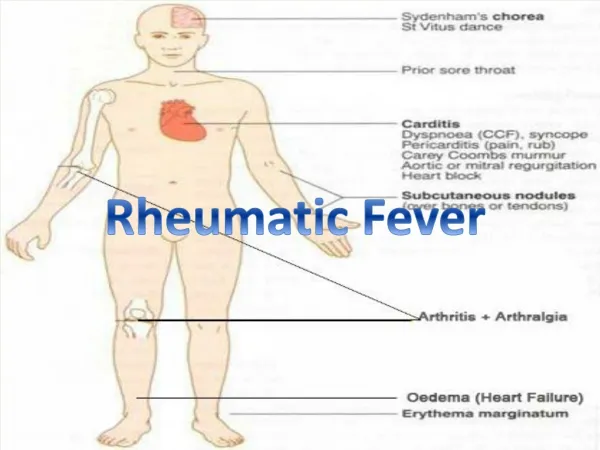
CLINICAL FEATURES Major Criteria: • Carditis • Polyarthritis, migratory • Erthema marginatum • Chorea • Subcutaneous nodules Minor criteria: • Fever • Arthralgia • Elevated acute phase reactants( ESR, CRP) • Prolonged PR interval in ECG Plus evidence of preceding group-A streptococcal infection (culture, rapid antigen, and antibody rise/elevation).Two major or one minor criteria or 2 minor criteria and plus evidence of preceding streptococcal infection indicate a high probability of rheumatic fever.
It occurs in 75% of cases. • Usual presentation with red, swollen, warm and tender joints and is migratory in nature. • Resolution of joint symptoms occurs in 6 weeks and seldom produces chronic joint disease. • In the last decade most common presentation was in the form of migrating arthralgia.
Firm • Painless • Freely movable • 0.5 to 2cm • Occipital area • Spinous processes • Extensor surface of the limbs
Rash • Evanescent • Erythematous • Macular • Non pruritic • Pale centers • Serpiginous margin • Trunk • Proximal estremties
CHOREA Even though it has been reported to occur as high as in 20% of patients, it is an uncommon manifestation in the present era.
MAJOR CRITERIA: • CARDITIS:Carditis occurs in 40-60% cases of rheumatic fever. 1. Valvulitis: • Valvular insufficiency commonly affecting Mitral Valve. • Carrey-coombs murmur, a sign of active mitral valvulitis. • Isolated aortic valvular involvement is rare and other valvular involvements are unusual.
Pericarditis • Manifested as chest pain, pericardial rub.
Myocarditis • Myocarditis manifests itself as disproportionate tachycardia, soft heart sounds, cardiomegaly, S3 congestive cardiac failure.
MINOR CRITERIA: • Fever:it ranges from 101-102 degree F. • Arthralgia:Diagnosed only in the absence of arthritis • Evidence of group A streptococcal infection:Positive throat culture or Elevated streptococcal antibodies ASO, Anti-DNAse B or antihyaluronidase
LABORATORY DIAGNOSIS: • Throat culture: Only 11% of the patients have positive throat culture for group A Streptococci. • Streptococcal antibody test: • ASO titre rise in 80% of patients • Anti DNAase –B and AH are indicators of recent streptococcal infection • Positive Streptozyme test • Acute phase reactants: ESR, CRP are raised in almost all patients • ECG: Prolonged PR interval is seen in ECG in carditis. tachycardia, AV block, QRS-T changes suggest myocarditis. • Chest radiography: Useful to assess cardiac size and pericardial effusion, pulmonary edema and increased pulmonary venous hypertension
Echocardiography • Useful in confirming endocardial, Myocardial and pericardial involvement and valve involvement. • Global hypokinesia of left and right ventricle walls • Multiple non-infectious verrucae over the atrial surface, atrio-ventricular valves and / or aortic valve. • Over the point of contact of leaflets. • Thickening of the valve leaflets • Trivial mitral and / or aortic regurgitation • Transient pericardial effusion and thickening of the epi-cardium can be observed.
Treatment • Arthritis: • Aspirin 100mg/kg/day is the drug of choice • Bed rest is advised. • Carditis: • In absence of congestive cardiac failure salicylates are beneficial otherwise prednisolone 1-2 mg/kg/day is given. • While tapering the dose of steroids after 4 weeks, salicylates has to be added and continued for 3-4 weeks to prevent rebound. • Syndenhams Chorea: Diazepam is sufficient in severe case haloperidol can be used. • Skin manifestations: No treatment is required
DURATION OF SECONDARY PROPHYLAXIS IN PATIENTS WITH RHEUMATIC FEVER
to conclude….. • High degree of suspicion • Throat infection with constitutional symptoms • Positive throat culture – GAS • Arthralgia • Penicillin • Rest