Download
1 / 31
310 likes | 533 Views
FUNNY LOOKING BEATS. CHAPTER 7. ESCAPE BEATS. ONE OR MORE EXTRA CARDIAC CYCLES ARE THE MOST COMMON ABNORMALITY IN AN EKG. CONDUCTION CELLS OUTSIDE THE SA NODE DEVELOP AN ABNORMALLY INCREASED AUTOMATICITY.

E N D
FUNNY LOOKING BEATS CHAPTER 7
ESCAPE BEATS • ONE OR MORE EXTRA CARDIAC CYCLES ARE THE MOST COMMON ABNORMALITY IN AN EKG. • CONDUCTION CELLS OUTSIDE THE SA NODE DEVELOP AN ABNORMALLY INCREASED AUTOMATICITY. • THE SA NODE IS UNABLE TO SUPPRESS THE INCREASED AUTOMATICITY BY NORMAL OVERDRIVE SUPPRESSION.
THE MOST AUTOMATIC CELL GENERATES A STIMULUS WHICH CAUSES A CONTRACTION, AND THE CELL BECOMES AN ABNORMAL PACEMAKER. INCREASED AUTOMATICITY IS CONSIDERED CARDIAC IRRITIBILITY BECAUSE IT IS UNDESIRABLE. THE EXTRA BEATS ARE UNDESIRABLE BECAUSE THEY MAY NEGATIVELY AFFECT CARDIAC OUTPUT. SA NODE SUPPRESSION CAUSING CARDIAC RATE SLOWING IS ANOTHER CAUSE FOR EXTRA BEATS. OVERDRIVE SUPPRESSION WEAKENS OR FAILS BECAUSE THE SA NODE IS NO LONGER THE MOST AUTOMATIC SITE IN THE CONDUCTION SYSTEM.
THE AUTOMATICITY SITE IN THE CONDUCTION SYSTEM MAY COMPETE TO OVERDRIVE THE FAILING SA NODE AND CAUSE A CONDUCTED IMPULSE. AN ECTOPIC FOCUS IS A SITE OF IMPULSE FORMATION LOCATED SOMEWHERE OTHER THAN THE SA NODE. ECTOPIC BEATS OR ECTOPY ARE EXTRA CONTRACTIONS IDENTIFIED BY THE LOCATION OF THEIR FOCI. ADDITIONAL NOMENCLATURE INDICATES THE PHYSICAL SITE OF THE FOCUS, DEFINING THE CONTRACTION AS ATRIAL, JUNCTIONAL, OR VENTRICULAR.
PREMATURE ECTOPY • ECTOPIC BEATS ARE CATAGORIZED BY THEIR TIMING IN THE EKG. • PREMATURE BEATS OCCUR IN THE EKG BEFORE THE NEXT REGULAR BEAT CAN OCCUR. • EXAMPLES: PAC, PJC, PVC • IDENTIFIABLE BY THEIR WAVES OF CONDUCTION RECORDED ON THE EKG.
ESCAPE ECTOPY • MAJOR FORM OF ECTOPY IS THE CONTRACTION WHICH OCCURS BECAUSE THE UNDERLYING RATE IS ABNORMALLY SLOW. • THESE CONTRACTIONS ARE A COMPENSATORY MECHANISM OF THE HEART FOR BRADYDYSRHYTHMIA.
THE SINUS RHYTHM IS DEPRESSED WITH A RATE SLOWER THAN 60 BEATS. NORMAL AUTOMATICITY OF THE OTHER CONDUCTION CELLS COMPETES WITH THE OVERDRIVE SUPPRESSION OF THE SLOWED SINUS RHYTHM. ALLOWS AN ECTOPIC FOCUS TO ESCAPE TO CAUSE A CONTRACTION. ANY ECTOPICS IN BRADYCARDIC RHYTHM ARE CLASSIFIED AS ESCAPE BEATS. ESCAPE ECTOPY IS COMPENSATORY MECHANISM FOR A SLOW RATE. PREMATURE ECTOPY INDICATES CARDIAC IRRITIBILITY.
MANAGEMENT OF THE PATIENT MUST CONSIDER THE UNDERLYING PATHOLOGY. ESCAPE ECTOPY IS MANAGED BY ADDRESSING THE BRADYCARDIA. PREMATURE ECTOPY IS MANAGED DIRECTLY WITH ANTIDYSRHYMIC THERAPIES.
PAC’S • PACEMAKER STIMULUS. • STIMULUS ARISES SOMEWHERE OTHER THAN THE SA NODE WITHIN THE TWO ATRIA. • ANY PREMATURE COMPLEX WITH A P WAVE WITHIN NORMAL LIMITS IS A PAC. • IF IT FAILS TO MEET THE CRITERIA IT IS CLASSIFIED AS ABERRANT PAC.
ATRIAL ECTOPY IS COMMON. IT DOES NOT RULE OUT THE PRESENCE OF SIGNIFICANT HEART DISEASE. MAY CONTRIBUTE TO TACHYDYSRHYTHMIA. PATIENTS WITH PAC’S FREQUENTLY REPORT A SENSATION OF PALPITATIONS OR HAVING “SKIPPED A BEAT”.
PJC’S • PACEMAKER STIMULUS ARISES FROM AN ECTOPIC FOCUS WITHIN THE JUNCTION. • P WAVE CAN BE ABSENT, INVERTED, RETROGRADE. • JUNCTIONAL CONTRACTIONS ARE MORE OMINIOUS AND SUGGEST UNDERLYING PATHOLOGY.
PVC’S • ECTOPIC FOCUS WITHIN THE VENTRICLES. • MOST OMINOUS OF ALL ECTOPIC BEATS. • INDICATE INCREASED IRRITIBILITY. • MAY BE TREATED WITH ANTIDYSRHYMIC MEDICATIONS.
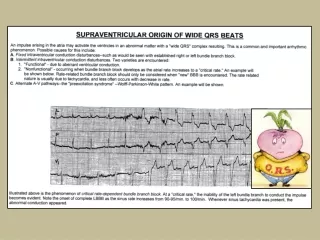
ABERRANT COMPLEXES • ONE VENTRICLE REPOLARIZES AT A SLOWER RATE THAN THE OTHER. • ONE VENTRICLE IS THEN ABLE TO ACCEPT AN ELECTRICAL IMPULSE CAUSING DEPOLARIZATION EARLIER THAN THE OTHER VENTRICLE. • INDIVIDUAL COMPLEXES THAT APPEAR DIFFERENT THAN THE COMPLEXES OF THE UNDERLYING RHYTHM.
THE ABERRANT COMPLEXES BECAUSE THEY DO NOT FOLLOW THE SAME ELECTRICAL CONDUCTION PATHWAY. ABERRANTLY CONDUCTED COMPLEXES INCLUDE AN ABERRANTLY CONDUCTED COMPLEX THAT HAS A NEGATIVE QRS WHEN THE UNDERLYING RHYTHM HAS A POSITIVE QRS COMPLEX. THE QRS OF THE ABERRANTLY CONDUCTED COMPLEX IS WIDER OR SHORTER THAN THE COMPLEXES OF THE UNDERLYING RHYTHM.
ABERRANTLY CONDUCTED COMPLEXES CAN ORIGINATE FROM ANYWHERE IN THE ATRIA, AV JUNCTION, OR VENTRICLES. THE ORIGIN WILL DETERMINE THE SIZE AND SHAPE. USUALLY OCCUR AS INDIVIDUAL COMPLEXES, NOT ENTIRE RHYTHMS.
PULSELESS ELECTRICAL ACTIVITY • DYSRHYTHMIA WITHOUT CONTRACTION OF THE MYOCARDIUM. • DEPOLARIZATION SEEMS TO OCCUR BUT NO PULSE OR B/P. • LETHAL AND TREATMENT MUST BEGIN IMMEDIATELY.
MAY BE CAUSED BY HYPOVOLEMIA, HYPOXIA, CARDIAC TAMPONADE OR TENSION PNEUMOTHORAX. PEA MAY OCCUR IF THE MYOCARDIUM IS SO DAMAGED IT CANNOT CONTRACT, ALTHOUGH ELECTRICAL IMPULSES ARE BEING CONDUCTED BY THE ELECTRICAL CONDUCTION PATHWAYS.
TEMPORARY PACEMAKERS • USED TO MAINTAIN HEART RATE IN AN EMERGENCY SITUATION OR UNTIL A PERMANENT PACEMAKER CAN BE SURGICALLY IMPLANTED. • TWO TYPES OF TEMPORARY PACEMAKERS.
TRANSVENOUS (THROUGH A VEIN). THE LEADWIRE IS INSERTED THROUGH THE SKIN AND THREADED THROUGH A LARGE VEIN INTO THE RIGHT SIDE OF THE HEART. ELECTRICAL IMPULSES STIMULATE THE ATRIUM AND THE IMPULSES ARE CARRIED THROUGH THE CARDIAC ELECTRICAL CONDUCTION SYSTEM, CAUSING DEPOLARIZATION. TRANSDERMAL OR TRANSCUTANEOUS (THROUGH THE SKIN). TWO LARGE PADS AS ELECTRODES CONDUCT THE IMPULSE.
TWO LEADWIRES EACH CONNECTED TO A PAD. ONE PAD ON THE FRONT AND ONE PAD ON THE BACK. THE IMPULSES ARE THEN CONDUCTED THROUGH THE BODY AND HEART STIMULATING THE ENTIRE HEART CAUSING DEPOLARIZATION. TRANSDERMAL IS EASILY POSITIONED AND DOES NOT REQUIRE PIERCING THE PATIENT’S SKIN TO POSITION THE ELECTRODES. FIXED PACEMAKER – GENERATES A CONSTANT RATE, 72 TO 80 IMPULSES. DEMAND – SET TO GENERATE IMPULSES ONLY WHEN THE PATIENT’S RATE FALLS BELOW A PREDETERMINED RATE.
PERMANENT PACEMAKERS • NECESSARY WHEN THE PATIENT IS UNABLE TO MAINTAIN A NORMAL HEART RATE OR CARDIAC OUTPUT, EVEN WITH AID OF MEDICATIONS. • GENERATOR IS SURGICALLY IMPLANTED UNDER THE PATIENT’S SKIN. • USUALLY UNDER THE UPPER LEFT CHEST SKIN OR ABDOMINAL AREA.
ATRIAL PACEMAKER • LEADWIRE AND ELECTRODE ARE INSERTED INTO THE RIGHT ATRIUM. • THE IMPULSE STIMULATES THE ATRIA, THEN FOLLOWS THE NORMAL ELECTRICAL PATHWAY. • THE DISCHARGE IS REPRESENTED BY A VERTICAL LINE CALLED A PACER SPIKE. • THE SPIKE IS USUALLY FOLLOWED BY A P WAVE AND QRS.
THE P WAVE MAY NOT BE SEEN UNLESS THE ELECTRODE IS POSITIONED HIGH IN THE RIGHT ATRIUM. THE P WAVE FOLLOWING A PACER SPIKE IS USUALLY NOT MEASURED. ATRIAL PACEMAKER CAN ONLY BE USED IF THE AV JUNCTION AND VENTRICULAR CONDUCTION PATHWAYS ARE FUNCTIONING. RARELY USED TODAY BECAUSE THEY ARE LESS EFFICIENT THAN VENTRICULAR OR SEQUENTIAL PACEMAKERS.
VENTRICULAR PACEMAKERS • THE LEADWIRE AND ELECTRODE ARE PLACED IN THE RIGHT VENTRICLE. • CAUSES DEPOLARIZATION OF THE VENTRICULAR MUSCLE. • THE ATRIA MAY NOT DEPOLARIZE IF THE ATRIAL MYOCARDIUM IS EXTENSIVELY DAMAGED. • A PACER SPIKE FOLLOWS THE QRS. • THE QRS IS USUALLY GREATER THAN 0.12 SECONDS.
SEQUENTIAL PACEMAKERS • COMMONLY USED. • STIMULATES THE DEPOLARIZATION OF BOTH THE ATRIA AND VENTRICLES. • THE LEADWIRE HAS TWO ELECTRODES – ONE IN THE ATRIA AND ONE IN THE VENTRICLE.
THE RHYTHM STRIP USUALLY SHOWS TWO PACER SPIKES BEFORE EACH QRS COMPLEX. SPIKES MAY OCCUR CLOSELY TOGETHER THAT THEY APPEAR AS ONE LONG SPIKE. FIRST SPIKE REPRESENTS THE ATRIA FIRING, THE SECOND REPRESENTS THE VENTRICLE FIRING. P WAVE MAY BE SEEN, AND QRS IS GREATER THAN 0.12 SECONDS.
CAPTURE AND PACING • THE PERCENTAGE OF CAPTURE AND PACING MUST BE DETERMINED. • CAPTURE REFERS TO THE CARDIAC MUSCLE’S ABILITY TO CONDUCT THE ELECTRICAL IMPULSE GENERATED BY A MECHANICAL PACEMAKER. • P WAVE OR QRS COMPLEX FOLLOWING EVERY PACER SPIKE.
THE PRESENCE OF A COMPLEX FOLLOWING A PACER SPIKE DOES NOT ALWAYS INDICATE THE CONTRACTION OF THE MYOCARDIUM, ONLY THE CONDUCTION OF AN ELECTRICAL IMPULSE. THE PATIENT MUST BE ASSESSED. PERCENTAGE OF CAPTURE IS DETERMINED BY THE NUMBER OF PACER SPIKES FOLLOWED BY A COMPLEX IN RELATIONSHIP TO THE TOTAL NUMBER OF PACER SPIKES ON THE ENTIRE STRIP. LOSS OF CAPTURE – A QRS DOES NOT FOLLOW A PACER SPIKE.
LOSS OF CAPTURE INDICATES THE ELECTRICAL IMPULSE GENERATED BY THE MECHANICAL PACEMAKER HAS NOT BEEN CONDUCTED. MAY INDICATE THE MYOCARDIUM IS SO DAMAGED, IT IS UNABLE TO RESPOND TO EVERY ELECTRICAL IMPULSE. PACING REFERS TO THE PERCENTAGE OF COMPLEXES GENERATED BY THE MECHANICAL PACEMAKER. THE PERCENTAGE OF PACING DEPENDS ON THE PACEMAKER ABILITY OF THE PATIENT’S OWN HEART THE PERCENTAGE OF CAPTURE SHOULD ALWAYS BE 100%.
AICD’S • AUTOMATIC IMPLANTABLE CARDIOVERTER DEFIBRILLATORS • CAN IDENTIFY AND TREAT SOME RAPID LETHAL DYSRHYTHMIAS. • SURGICALLY IMPLANTED. • CAN BE PROGRAMMED TO INITIATE LOW-VOLTAGE ELECTRICAL IMPULSES WHEN THE HEART RATE BECOMES VERY FAST.
THE AICD IMPULSE ATTEMPTS TO FORCE THE HEART INTO A NORMAL RATE. IF THE HEART RATE CONTINUES TO INCREASE, OR IF THE RHYTHM BECOMES V-FIB OR V-TACH, THE AICD WILL DELIVER A SHOCK STRONG ENOUGH TO DEFIBRILLATE. THE AICD WILL DEFIBRILLATE THE PATIENT UNTIL THE HEART HAS RECOVERED OR UNTIL IT IS TURNED OFF BY MEDICAL PERSONNEL. ON THE RHYTHM STRIP, THE FIRING OF THE AICD APPEARS SIMILAR TO A PACING SPIKE, BUT MAY HAVE A GREATER AMPLITUDE.