Download
1 / 1
20 likes | 377 Views
Using Episodes of Care to Analyze Asthma in Utah Medicaid Risk Groups & Scores Demographic Prospective Retrospective Cost Summary by Episode ETG/ERG Episode Treatment Groups Analysis Claims FFS & Encounter EPG Episode Prescription Groups Risk Groups & Scores Demographic

E N D
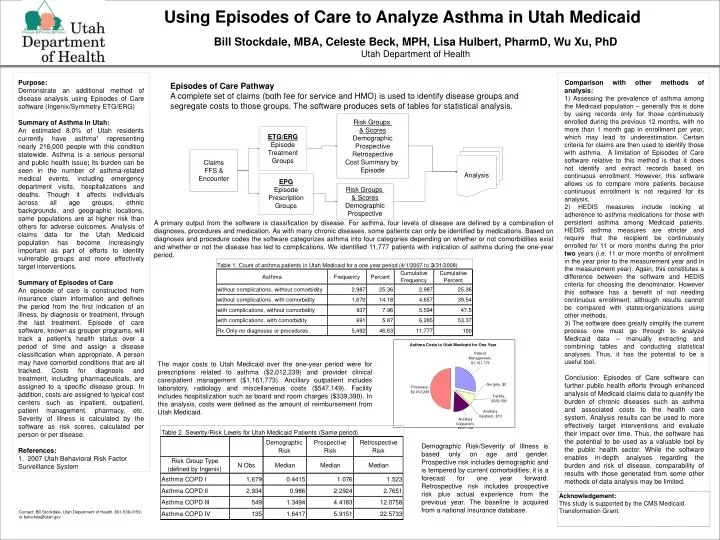
Using Episodes of Care to Analyze Asthma in Utah Medicaid Risk Groups & Scores Demographic Prospective Retrospective Cost Summary by Episode ETG/ERG Episode Treatment Groups Analysis Claims FFS & Encounter EPG Episode Prescription Groups Risk Groups & Scores Demographic Prospective • Bill Stockdale, MBA, Celeste Beck, MPH, Lisa Hulbert, PharmD, Wu Xu, PhD • Utah Department of Health Purpose: Demonstrate an additional method of disease analysis using Episodes of Care software (Ingenix/Symmetry ETG/ERG) Summary of Asthma in Utah: An estimated 8.0% of Utah residents currently have asthma1 representing nearly 216,000 people with this condition statewide. Asthma is a serious personal and public health issue; its burden can be seen in the number of asthma-related medical events, including emergency department visits, hospitalizations and deaths. Though it affects individuals across all age groups, ethnic backgrounds, and geographic locations, some populations are at higher risk than others for adverse outcomes. Analysis of claims data for the Utah Medicaid population has become increasingly important as part of efforts to identify vulnerable groups and more effectively target interventions. Summary of Episodes of Care An episode of care is constructed from insurance claim information and defines the period from the first indication of an illness, by diagnosis or treatment, through the last treatment. Episode of care software, known as grouper programs, will track a patient’s health status over a period of time and assign a disease classification when appropriate. A person may have comorbid conditions that are all tracked. Costs for diagnosis and treatment, including pharmaceuticals, are assigned to a specific disease group. In addition, costs are assigned to typical cost centers such as inpatient, outpatient, patient management, pharmacy, etc. Severity of illness is calculated by the software as risk scores, calculated per person or per disease. References: 1. 2007 Utah Behavioral Risk Factor Surveillance System Comparison with other methods of analysis: 1) Assessing the prevalence of asthma among the Medicaid population – generally this is done by using records only for those continuously enrolled during the previous 12 months, with no more than 1 month gap in enrollment per year, which may lead to underestimation. Certain criteria for claims are then used to identify those with asthma. A limitation of Episodes of Care software relative to this method is that it does not identify and extract records based on continuous enrollment. However, this software allows us to compare more patients because continuous enrollment is not required for its analysis. 2) HEDIS measures include looking at adherence to asthma medications for those with persistent asthma among Medicaid patients. HEDIS asthma measures are stricter and require that the recipient be continuously enrolled for 11 or more months during the prior two years (i.e. 11 or more months of enrollment in the year prior to the measurement year and in the measurement year). Again, this constitutes a difference between the software and HEDIS criteria for choosing the denominator. However this software has a benefit of not needing continuous enrollment, although results cannot be compared with states/organizations using other methods. 3) The software does greatly simplify the current process one must go through to analyze Medicaid data – manually extracting and combining tables and conducting statistical analyses. Thus, it has the potential to be a useful tool. Conclusion: Episodes of Care software can further public health efforts through enhanced analysis of Medicaid claims data to quantify the burden of chronic diseases such as asthma and associated costs to the health care system. Analysis results can be used to more effectively target interventions and evaluate their impact over time. Thus, the software has the potential to be used as a valuable tool by the public health sector. While the software enables in-depth analyses regarding the burden and risk of disease, comparability of results with those generated from some other methods of data analysis may be limited. Episodes of Care Pathway A complete set of claims (both fee for service and HMO) is used to identify disease groups and segregate costs to those groups. The software produces sets of tables for statistical analysis. A primary output from the software is classification by disease. For asthma, four levels of disease are defined by a combination of diagnoses, procedures and medication. As with many chronic diseases, some patients can only be identified by medications. Based on diagnoses and procedure codes the software categorizes asthma into four categories depending on whether or not comorbidities exist and whether or not the disease has led to complications. We identified 11,777 patients with indication of asthma during the one-year period. The major costs to Utah Medicaid over the one-year period were for prescriptions related to asthma ($2,012,239) and provider clinical care/patient management ($1,161,773). Ancillary outpatient includes laboratory, radiology and miscellaneous costs ($547,149). Facility includes hospitalization such as board and room charges ($339,390). In this analysis, costs were defined as the amount of reimbursement from Utah Medicaid. Demographic Risk/Severity of Illness is based only on age and gender. Prospective risk includes demographic and is tempered by current comorbidities; it is a forecast for one year forward. Retrospective risk includes prospective risk plus actual experience from the previous year. The baseline is acquired from a national insurance database. Acknowledgement: This study is supported by the CMS Medicaid Transformation Grant. Contact: Bill Stockdale, Utah Department of Health, 801-538-9159, or bstockda@utah.gov