Download
1 / 12
120 likes | 277 Views
Reducing Avoidable Re-Hospitalizations and Improving Care Transitions. National Academy for State Health Policy October 4, 2011 Pam Coleman INSPIRIS.

E N D
Reducing Avoidable Re-Hospitalizations and Improving Care Transitions National Academy for State Health Policy October 4, 2011 Pam Coleman INSPIRIS
75% of all 30-day hospital re-admissions of Medicare patients in 2005 were potentially preventable — or 13% of total admissions. If these re-admissions were eliminated, Medicare could save $12 billion annually. One-in-six Medicaid members with three or more underlying health problems is re-admitted within 30 days. For the ABD population, that number is between 16% and 23%. Hospitals are not currently penalized for readmissions – in fact they are paid for each admission Nursing facilities have a financial incentive to admit dual eligibles to hospitals so they can return under Medicare status The Problem 2
Re-admissions Targeted in ACA • The Affordable Care Act (ACA) focuses on holding care providers responsible and of managing health care spending. • ACA gave CMS the authority to penalize hospitals for excess re-admission, focusing initially on heart failure, acute myocardial infarction and pneumonia. • CMS can withhold up to 1% of all inpatient Medicare payments starting in FFY 2013, up to 2% of payments in FFY 2014 and up to 3% in FFY 2015 and thereafter. 4
The Solution: • “To control what is happening with these patients (and thus reduce costs) you must watch them like a hawk, and be ready, willing and able to get involved in all sorts of creative ways at almost any moment.” • Dr. Peter Boling, Past-President, AAHCP and • Chairman, Internal Medicine, Medical College of Virginia 5
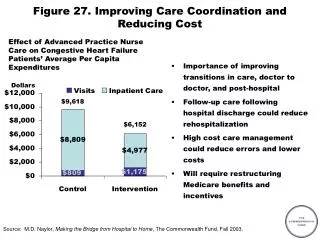
In-Home Primary Care Program Enhanced quality, satisfaction, reduced medical expenses driven by three pillar approach Proactive care and care management – regular visits from home visiting provider to improve patient care and reduce number of exacerbations Urgent visits as needed to provide immediate access to a provider when exacerbations do occur-also a heavy focus on reducing readmissions with visits within 48-72 hours of a hospitalization Focus on advance directives & end of life education 6
Transitions Strategies Depend on the Individual’s Needs Transition coaching (RN) Telephonic nurse care manager Provider visit (High Risk) Comprehensive clinical assessment Environmental assessment and confirmation of information obtained by Provider available for follow-up visits Coordination with existing health plan programs Program duration and scope customized to plan needs 7
Transition Services Medication reconciliation Review of discharge instructions Assessment of caregiver support system Confirmation of DME, home nursing and rehabilitation services Opportunity for review of eligibility for other INSPIRIS/health plan services Complete assessment 8
Transitions – Home Setting Reduction in Re-admissions 9 9
Program Impact on Total Costs & Key Utilization Metrics – Medicaid Plan (SSI Population) 11
Dual Eligible Model Concept to Reduce Hospital and NF Re-admissions • Integration model combining Medicare home based primary care with Medicaid long term services and supports (LTSS). • Target duals at risk for hospital and NF admissions • Primary care and LTSS are provided where the member lives utilizing a person-centered medical home approach. 12